![]()
The nutritional status of tribal and Bengali children under the age of five at Chattogram Hill Tracts in Bangladesh
Mohammad Nasir Uddin1*, A. S. M. Sharifur Rahman2, M. Ismail3, A. Nasrin4, Tahmina Bhuiyan5, Ariful Islam6
1Department of Zoology, University of Chittagong, Chittagong, Bangladesh; 2Department of Zoology, Noakhali Science and Technology University, Noakhali, Bangladesh; 3Department of Zoology, University of Chittagong, Chittagong, Bangladesh; 4Department of Pharmacy, State University, Bangladesh; 5Department of Zoology, Gurudayal Government College, Kishoreganj, Bangladesh; 6Green Banking Officer (Data center), Bangladesh
ABSTRACT
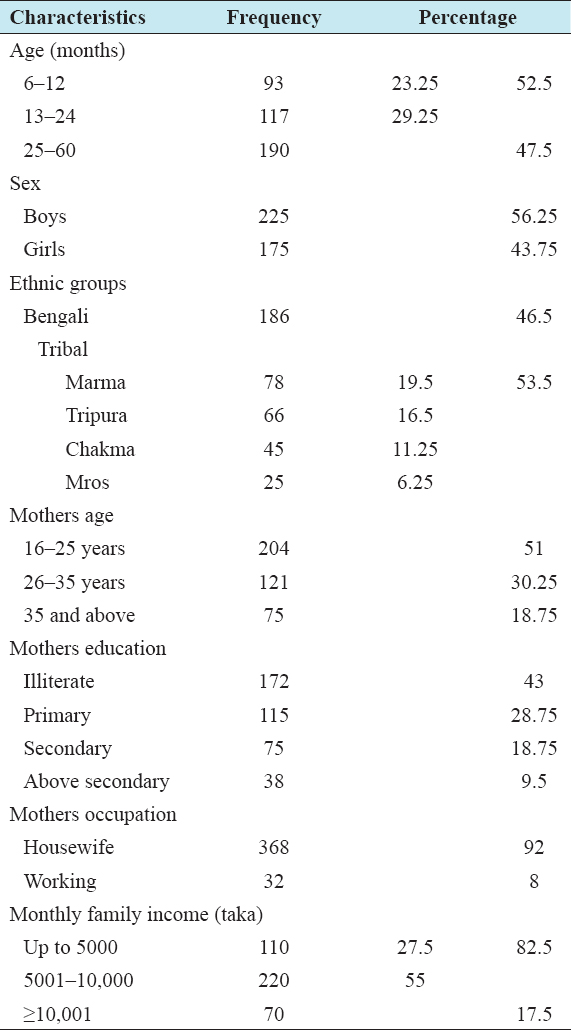
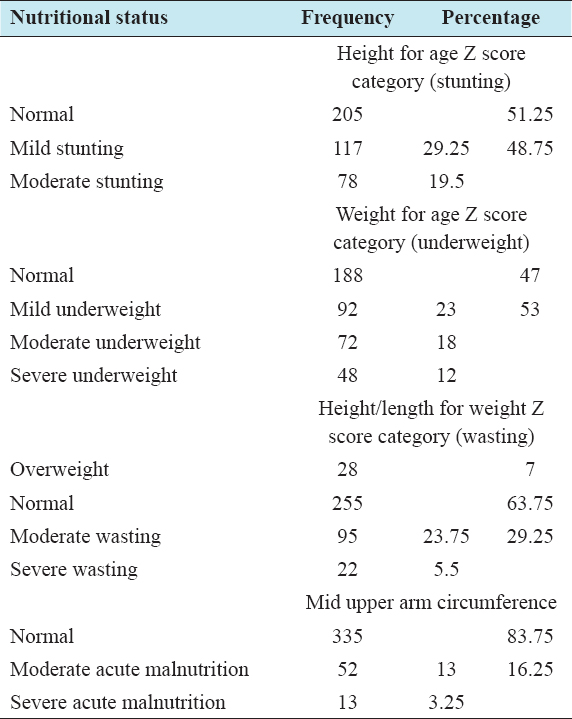
Adequate nutrition during infancy and early childhood is fundamental to the development of child’s full human potentials. Malnutrition is recognized as one of the major causes of morbidity and mortality among the children under-5 years and developing countries are the worst affected. This paper investigates the nutritional status of under-5 children of the Chattogram Hill Tracts who are culturally different from the plain land population. Analysis of nutritional status data shows that out of 400 children, 56.25% were boys, 43.75% were girls, and 52.5% were aged <2 years. About 53.5% of children were tribal and 46.5% were Bengali. Majority (51%) of the children’s mothers’ age was below 25 years, 43% was illiterate, 92% were housewives, and 82.5% had monthly family income that was <10,000 taka. Regarding children nutritional status, 19.5% was moderate stunted, 29.25% was mild stunted; severe, moderate, and mild underweight were 12%, 18%, and 23%, respectively. About 5.5% was found severe wasted and 23.75% was moderate wasted. By mid upper arm circumference, 13% were of moderate acute malnutrition and 3.25% were of severe acute malnutrition.
Keywords: Bangladesh, Chattogram Hill Tracts, ethnic minorities, nutritional status