INTRODUCTION
Aggression is best described as any form of action pointed to the target of hurting or damaging another living being who intends to avoid such action.[1] Aggression is extensive[2] and develops from childhood to adolescence,[3,4] and health outcomes associated with damage across countries are similar.[5] Both aggression perpetration and victimization increase the risks of externalizing and internalizing problems in adolescents.[6-8]
In recent years, a series of vicious incidents occurred in campuses of China and caused irreparable loss for school, family, and society. China’s domestic survey showed that 17.98% of the college students reported that they had ever experienced campus violence in the most recent year.[9] In Beijing, the number of criminal detention of college students in 2005 is 3.8 times that of 2000, and the number of college students’ crime increased by 28.2%.[10] Since 1999, the quantity of Chinese College students’ crime related to aggression increases year by year.[11,12]
High aggression is associated with violent crime,[13-16] and effective reducing aggression level will be effective in preventing violent crime.[17,18] As far as development trend is concerned, there is imbalance between theory study and practice of aggression intervention. Scholars realize the presence of a gap between aggression theory and practice.[19] In Mainland China, studies of intervention on aggression among college students are very few at present. Most researches belong to the preliminary discussion from the perspective of theory. For example, Chen and Qu[20] discussed “experience of positive emotion” applying to control undergraduates’ violence on the basic of “emotion and violence” and “the function of positive emotion” theories. Another study showed that dialectical thinking leads to reduced aggression.[21] Therefore, at present and in Mainland China, it is more necessary for researchers to carry out an increasing number of researches of intervention for aggression.
Cognitive behavioral therapy (CBT) is derived from the integration of cognitive therapy and behavioral therapy. CBT is a kind of widely empirical support treatment for a mass of mental health problems including aggression.[22-24] For aggression, tactics used in a CBT way alter aggressive behavior while synchronously change their cognition about situations. It is suggested that aggression is associated with a tendency to interpret situations as threatening or hostile even when they are not. A goal of CBT is to reduce these kinds of hostile biases.[25] According to a meta-analysis of CBT in the intervention of aggression as well as hyperactivity-impulsivity, Robinson et al.[26] found that CBT was an effective treatment to reduce hyperactivity-impulsivity and aggression in children and youth. CBT supposes that changing maladaptive thinking can change the emotion and behavior,[27] but recent variants emphasize changes in one’s relationship to maladaptive thinking rather than changes in thinking itself.[28] CBT is characteristically concise, collaborative, problem-focused, and goal-oriented. It focuses on defining the problem, generating alternative solutions, anticipating consequences, introducing behavioral monitoring, and prioritizing responses. Everyone has his/her own special cogitation pattern which is affected by individual experiences, faith, and schemas. Distortions of cognition promote persons’ misunderstanding of actuality, paying more attention to negative indications, or bring to mind the negative state of affairs, which promote negative schemas of the world, the self, and future.[29] CBT concentrates on making better emotive responses and maladjusted actions by altering cognitions.[30] CBT is described as remedial actions, combining tactics from cognitive and behavior psychology to intervene varying disorders such as fear, anxiety, phobia, and aggression.[24] As mentioned above, a cognitive viewpoint of aggression considers that aggression is manifestation of a person’s irrational thoughts. These thoughts lead to hostility, anger, and aggression.[31] Conventionally, CBT is mostly used in individual treatment. With the growing number of psychological disorders, the phenomenon of a lack of professional therapists is more prominent. As a result, more and more researchers gradually turn to pay close attention to group CBT. Researchers found that under the same condition of treatment time, the efficiency of the group therapy is 50% more efficient than individual therapy. At the same time, the group therapy can reduce the economic costs.[32]
Cognitive restructuring has been successfully used in the treatment of aggression. Aderanti and Hassan[33] investigated the effectiveness of cognitive restructuring and self-management on adolescent rebelliousness. The finding proved that cognitive restructuring was effective in the treatment of rebelliousness. Shirin et al.[34] investigated the potency of the program of anger management on decreasing the aggression among middle school students. The outcomes showed that the program of anger management could reduce total aggression, aggressive behavior, and thought of aggression in high school students. Problem-solving skill training is a kind of cognitive behavioral intervention which pays attention to train the adaptive attitudes and skills to solve the social problem. Social problem solving is thought to play an important role as a mediator and host the relationship between the stressful life events and happiness.[35] Deficit in problem-solving skills plays an important role in the progress of aggression.[36] Rebecca[37] investigated the impact of a social problem-solving skills’ training program with a sample of 105 juvenile offenders. The result showed that the adolescents in the intervention conditions significantly improved on their aggressive behavior from before and after the intervention compared with adolescents in the control condition. Besides, studies showed that social skills’ training significantly increased social growth, self-esteem, personality adequacy, and reduced inappropriate behaviors such as aggression in adolescents.[38-44]
Aggression is thought to reflect a defect in integrating brain structures and promoting emotion regulation,[45] moral decision-making[46] and utilization of knowledge about social conventions.[47] Interpersonal provocation usually enhances aggressive impulses and anger. Failed to master impulse of aggression is often a general reason of violence and aggression.[48] Baumeister et al.[49] defined self-control as the capacity of regulating cognition, emotion, and behavior for the sake of achieving long-range targets. Matt[50] defined self-control as the ability to control one’s emotions, behavior, and desires in the face of external demands to function in society. Tangney et al.[51] proved that people with high self-control had more satisfying and secure interpersonal relationships and less aggression than people with low self-control.
The implication of social support is the network of all people with whom a person has family, social, and personal relations.[52] Social support includes four primary classifications - instrumental, social, informative, and emotional. Bandura[53] emphasizes that children or adolescents’ social network is a major factor in prediction of whether they will turn into aggressive or not. The adolescent, who has positive company and fine social network, is able to generate a sociable trend instead of antisocial action. Therefore, social support is a major part of the resources of environment for young people. Rajesh et al.[54] conducted a study to investigate the impact of social support on self-esteem and aggression. The result showed that there was a significant negative correlation between aggression and social support (r = −0.22). From the literature, pressure and distress are the most common causes of aggression.[55,56] Kashani and Shepperd[57] conducted a study to determine the degree of social support in predicting the adolescents’ using reasoning and aggression to solve the interpersonal conflict. Despite all the teenagers appeared to use reasoning to solve the conflict, those with a low level of social support were more likely to report using verbal and physical aggression to resolve conflict. Kase et al.[58] investigated the relationships between aggression, life skills, social support, and mental health. Covariance structure analysis showed that the life skills scores were positively related to the social support scores, and then, the social support scores were negatively related to the aggression scores.
Based on the existing studies, the researcher creatively adopts optimized integration of a variety of cognitive behavioral skills to make the treatment plan of more reasonable. Group CBT (G-CBT) adopts the same basic structure and focus of individual CBT, though modifies to employ the group format. Relative to the individual therapy, group psychotherapy could solve more similar psychological barriers in the same time. A group provides clients with a platform which is closer to the real world, facilitated transferring the acquired skills to real life. In view of the current station of a lack of professional mental health workers in Chinese universities, to a certain extent, this study should provide an approach to make up for the shortage. At the same time, this study should further broaden the applicatory field of CBT and provide new empirical support for the related theories of psychotherapy.
Hence, the purpose of this study was to examine three hypotheses: (1) The G-CBT is effective in treating aggression and the effect is stable; (2) the G-CBT is effective in enhancing self-control and the effect is stable; and (3) the G-CBT is effective in improving social support and the effect is stable.
METHODS
Design
As an experimental study, the design of this study was randomized pre- and post-test with control group design. The researcher respectively investigated the short-term effect and long-term effect of G-CBT for aggression, self-control, and social support. To eliminate or control the influence of extraneous variables as much as possible, the researcher did a series of arrangement in experimental design. For example, the three universities to which participants belonged located in the same city, and thus, it could effectively reduce the effect of regional difference to the result. Besides, this study was a long-term intervention study, and the subjects lived and studied under natural conditions except participating in the regular treatment. To control the additional variables which might cause psychological and behavioral changes of the subjects, a control group was set. All treatments were arranged in the same place, and the researcher as well as the assistants who participated in this study had accepted the unified training and adopted the same treatment program. Due to random sampling and the existence of the control group, the research could effectively prevent the selective bias, avoid the participation of subjective factors, control the systemic error, balance the influence of unexpected factors, and be the basis of inference statistics. Moreover, the questionnaires which were used in this study had higher reliability and validity, and these three questionnaires were consistent in the three measures. For the sake of preventing the influence of memory which was formed in the previous tests on the subsequent tests, the researcher added in two other questionnaires, one is Eysenck personality questionnaire, and the other is 16 personality factor questionnaire (16 PF). Therefore, the effects of instrumentation for this study could be controlled.
Participants
The target population of this study was the first grade students of three universities in Hebei province of China, which contained a comprehensive university, a university of medical sciences, and a normal university, and age between 18 and 19-year-old. There were a total of 8853 university students who met the requirement of this study. After stratified random sampling, a total of 1469 students were obtained. The main basis of stratified sampling in this study included gender (male or female) and professional fields (liberal arts or science). Through assessment using the questionnaire of Chinese College Students’ Version of Buss–Perry Aggression Questionnaire (CC-BPAQ), the participants whose score achieved aggressive evaluation standard (one standard deviation [SD] more than average) were selected. In accordance with random way, 60 subjects (male=26 and female=34) were extracted and averagely divided into two groups - the G-CBT group and the control group.
Baseline Equivalence
For the basic demographic characteristics such as age, gender, and so on, there was no significant difference between the two groups (P > 0.05). The total score of CC-BPAQ was the most important baseline index. The researcher had also checked the consistency of total score of self-control and social support between the treatment group and control group.
T-test between the control group and the G-CBT showed that in terms of total score of aggression, self-control, and social support, there was no significant difference (aggression: T = −0.719, P > 0.05; self-control: T = −1.769, P > 0.05; and social support: T = 0.947, P > 0.05). In other words, the baselines of total aggression, self-control, and social support were consistency and that implied the participants were homogeneous. In addition, this study was a single factor, repeated measurement design. Therefore, the intervention effect could be examined through, respectively, comparison the data of the measurements of the control group and the G-CBT group.
Procedure
The researcher had accepted the professional training of G-CBT and had obtained the corresponding qualification. The participants who took part in the intervention needed to meet the criteria of (1) getting high scores in aggression questionnaire and (2) agreeing participate in this study and having the willingness of enhancing own mental health. All participants needed to sign the informed consent.
In this study, the program of G-CBT referenced to several programs of aggression intervention such as aggression replacement training[59] and was carried out a certain adjustment. It involved 16 weekly sessions, each group included 10 participants and each session lasted for 60 min, while subjects in the control group did not receive any intervention, just to participate the assessments. All subjects were asked to complete the assessment for 3 times: Pre-test (1 week before the intervention), post-test 1 (1 week after the intervention), and post-test 2 (tracking), which was 4 months after intervention. This intervention involved four phases: (1) Pre-treatment assessment, (2) cognitive restructuring and moral reasoning (reconceptualization), (3) anger management, and (4) skills consolidation, application, and generalization.
Pre-treatment assessment was the initial phase of therapy and was in the form of individual. The therapist established the preliminary therapeutic alliance with clients, completed an assessment, and evaluated the client’s suitability for G-CBT. This process was completed before the formal treatment. In cognitive restructuring and moral reasoning (session 1–8), first, through a series of group activities such as “the wind blows”, “snowball,” and so on, the researcher (leader) promoted the group members’ knowing and understanding each other, clarified the goal and the nature of the group, and formed the expectation as well as the deed of the group. Second, the researcher helped the group members to understand the relationship between automatic thinking, emotion, and behavior; the concept and characteristics of anger and aggression; and learn empathy or transpositional consideration through the role playing of “the blinds and crutches” or “trip to trust.” Third, under the guidance of the leader, the group members understood their dominant characteristics of emotion and the characteristics of cognitive distortions. Through combing mood and discussion, the leader made the group members more adept at identifying automatic thoughts and experienced the changes of cognition and mood after setback. Fourth, the leader helped the team members to realize their negative emotions and the cause such as anger, the common forms of cognitive distortion, and preliminary master the rational thinking methods. Finally, through the group activity such as “dark map versus light map,” the leader helped the group members familiar with individual irrational beliefs, learn to change mood through adjusting cognition, understand the relationship between the automatic thinking, intermediate thinking and schema, and master cognitive restructuring techniques. In anger management stage (session 9–13), first, through role play, discussion and group activities, the leader helped the group members recognize the influence of anger for behavior, body and mind, the manifestations and characteristics of aggression, understand the basic methods for controlling negative emotions such as the effective method of venting and expressing anger through learning relaxation and biofeedback technology. Second, through a series of activities, the leader made the team members familiar with the principle of biofeedback and gradually master relaxation techniques, the problem-solving skills as well as effective communication techniques, accurately grasp the individual irrational beliefs, and skillfully use thinking conversion technology. Finally, through reviewing the transformation of thinking, relaxation, problem-solving, and social skills training, the researcher helped the group members more clearly understand their own problem orientations and problem-solving styles, familiar with effective communication skills, and develop well social skills. In skills’ consolidation, application, and generalization stage (session 14–16), first, the researcher further strengthened the group members’ adjustment methods and techniques of mood and helped them learn to build a cheerful mood and realize that they were the owners of mood. Second, through review, the group members listed strategies that they had learned and utilized to cope with aggression and anger in previous group activities, enhanced the understanding and mastering of these knowledge and skills, and discussed with the leader about the ways in which they could continue to use these techniques to manage future situations and events. Finally, the group members summarized their group experience and understood each group member’s performance in the group, and then, the leader finished the intervention friendly and safely.
In addition, the leader assigned the homework to the group members in every session except the last one and checked the completion of the homework at the beginning of each session. The fact proved that this process was very meaningful.
Measure
Aggression
CC-BPAQ was used in this study to measure aggression of the participants. CC-BPAQ includes 22 items and belongs to self-report, five-point Likert scale.[60] It is the Chinese revision of the BPAQ. The BPAQ is one of the most used instruments to assess aggression. In terms of the construct validity of CC-BPAQ, confirmatory factor analysis showed that the data fitting was good (goodness of fit index [GFI] = 0.917, adjusted GFI = 0.896, comparative fit index [CFI] = 0.899, and root mean square error of approximation [RMSEA] = 0.059). In terms of criterion validity, the scores of physical aggression, hostility, and anger proneness in CC-BPAQ negatively correlated with the scores of the Chinese University students social skill inventory (r = −0.19, −0.23, and −0.20; P < 0.01) while positively correlated with the scores of the revised cheek and buss shyness (r = 0.45, 0.21, 0.11, and 0.32; P < 0.01). In terms of the internal consistency, α of total score was = 0.89, and α of 4 subscales were between 0.73–0.85. The test-retest coefficient was 0.91 for the total scale and 0.75–0.80 for the 4 subscales (P < 0.01).[60]
Self-control
Self-control scale (SCS) for Chinese college students was used in this study to measure self-control of the participants. Tangney et al.[51] introduced a reflective measure of self-control which has gained popularity in social science research. Tangney demonstrated that their self-report scale of self-control items is correlated with a variety of individual behaviors and psychological well-being, including eating disorders, alcoholism, anxiety, depression, emotional stability, family conflict, and interpersonal relationship quality. The Chinese revised questionnaire still retains the three dimensions of impulse control, work or entertainment moderation, and resistance of temptation. The total variance explanation of the original questionnaire of five dimensions is 42.3% and the revised questionnaire is 53.7%.[61] Confirmatory factor analysis showed that the revised SCS was five-factor construct and had good construct validities (RMSEA = 0.050, GFI = 0.91, incremental fit index = 0.93, non-normed fit index (NNFI) =0.91, and CFI = 0.93). The correlation between total score of SCS and that of grade point average was 0.146; the correlation between total score of SCS and that of interpersonal satisfaction scale was 0.280; the correlation between total score of SCS and that of life satisfaction scale was 0.163, and the correlation between total score of SCS and that of general health questionnaire (CHQ) was 0.317. Internal consistency: α value for the SCS scale was 0.862. The reliability coefficient of the test-retest stability coefficient was 0.850.[61]
Social support
Social support scale for university students was used in this study to measure the social support of the participants. It is a rating scale that is suitable for Chinese College students and is formulated by Ye and Dai.[62] It contains 17 items that respectively belong to three factors - subjective support, objective support, and utilization degree. Confirmatory factor analysis showed that the values of NFI, NNFI, and CFI were above 0.9, RMSEA = 0.03. Using SCL-90 for criterion, the results showed that the test accords with the requirement of psychometrics. The internal consistency of the three subscales - subjective support, objective support, and support utilization degree in the college student samples, respectively, is 0.845, 0.814, and 0.874. For full scale, α = 0.906. The test-retest reliability coefficient of the three subscales and full scale are 0.630, 0.799, 0.720, and 0.821.
Data Analysis
The methods of statistical analysis adopted in this study mainly included Mauchly’s test of sphericity, single factor, repetitive measure analysis of variance, and T-test. All data analysis processes were finished using the Statistical Package for the Social Sciences (version 22).
RESULTS
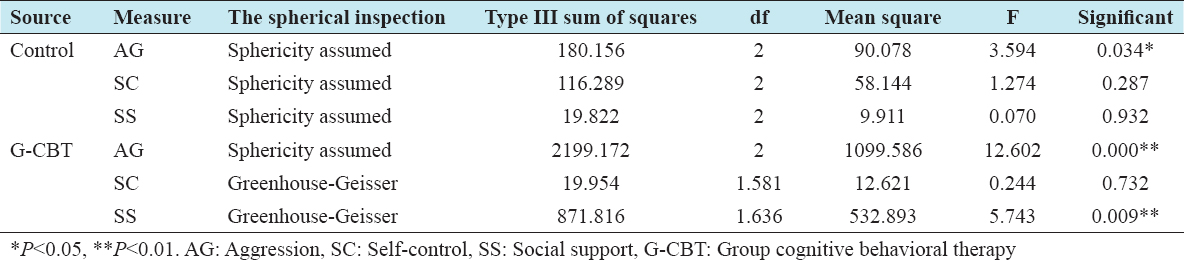
Table 2 displays the means and SDs of the total score of aggression, self-control, and social support by the time series. Spherical test results showed that some factors were significant, and the corrected values were adopted [Table 3]. Table 4 shows that in terms of control group, compared with pretest, there was a significant change on the total score of aggression, and the total score of aggression had dropped significantly (F = 3.594, P < 0.05); there was no significant change on the total score of self-control and social support. In terms of the G-CBT group, compared with pretest, there were significant differences on total score of aggression and social support. The total score of social support had increased significantly (F = 5.743, P < 0.01), and the total score of aggression had dropped significantly (F = 12.602, P < 0.01). Based on this, the researcher carried on the further examination for these dependent variables.
Table 1: Descriptive statistics of the total score of aggression, self-control, and social support
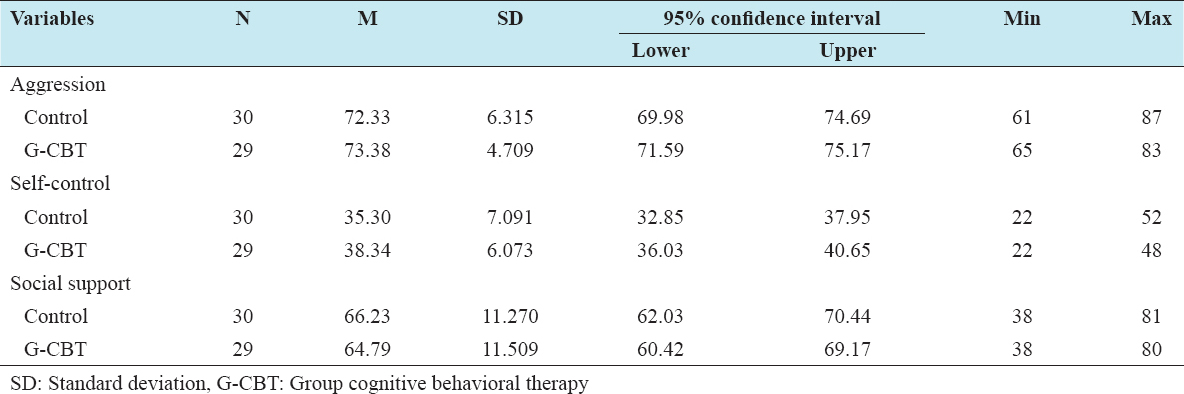
Table 2: Descriptive statistics of total aggression, self-control, and social support (time series)

Table 3: Mauchly’s test of sphericity for total aggression and social support
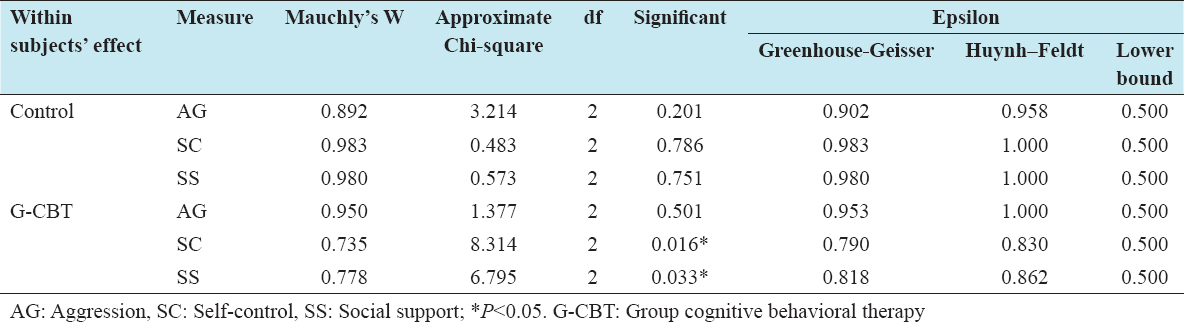
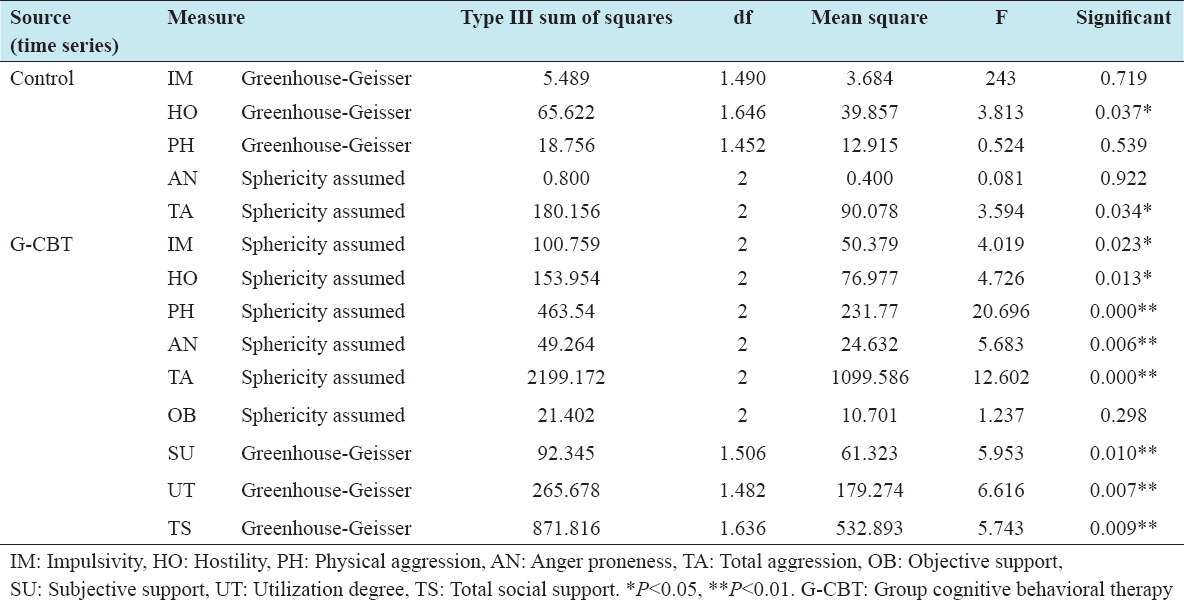
Table 4: Univariate Tests of total aggression, self-control, and social support (time series)
Tables 5 and 6 show that, for the control group, combined with time series and descriptive statistics, the hostility factor and total score had a significant difference between pre-test, post-test 1, and post-test 2 (P < 0.05). Hostility score decreased significantly in the post-test 1 but rebounded in the post-test 2. The total score showed a trend of decline. For the G-CBT group, the univariate tests of aggression showed that there were significant differences on the total score and the scores of all subscales between pre-test, post-test 1, and post-test 2 (impulsivity, F = 4.019, P < 0.05; hostility, F = 4.726, P < 0.05; physical aggression, F = 20.696, P < 0.01; and anger proneness, F = 5.683, P < 0.01). Combined with the descriptive statistics, the implementation of the G-IPT significantly reduced all subscales score, which further reduced the total score of aggression. The univariate tests of social support showed that there were significant differences on the total score and the subscales of subjective support and utilization degree between pre-test, post-test 1, and post-test 2 (subjective support, F = 5.953, P < 0.01 and utilization degree, F = 6.616, P < 0.01). Combined with the descriptive statistics, the implementation of the G-CBT significantly increased the subjective support, utilization degree, and total social support.
Table 5: Means and standard deviations of dependent variables by time series
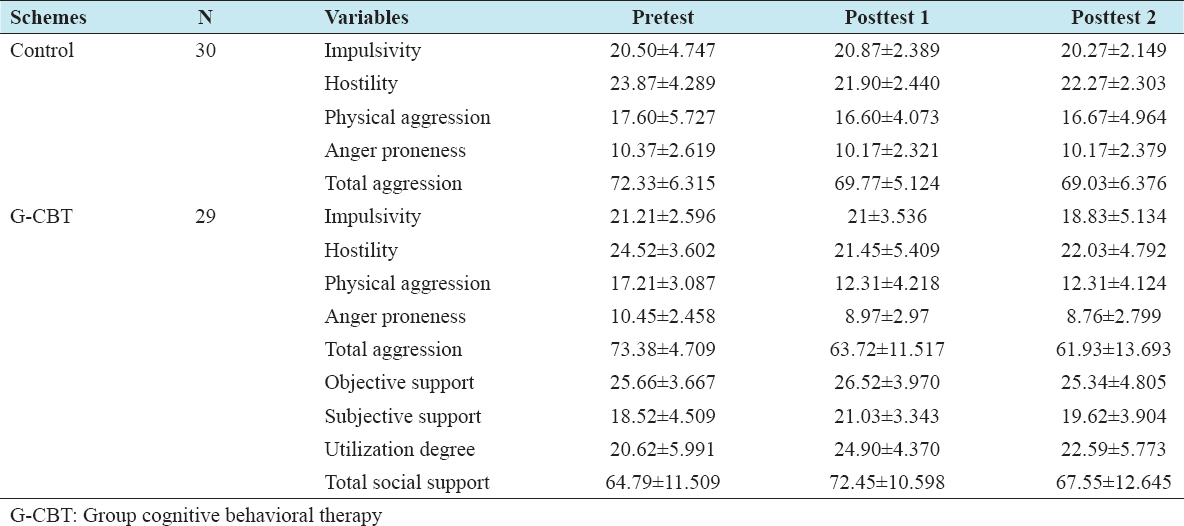
Table 6: Univariate Tests of dependent variables
By comparing the total aggression and social support of post-test 1 and post-test 2 between the two groups, there were significant differences between the G-CBT group and the control group. Except the total social support in the post-test 2 (T = 0.056, P > 0.05), the total aggression of the G-IPT group was significantly lower than the control group both in the post-test 1 (T = 2.619, P < 0.01) and post-test 2 (T = 2.568, P < 0.01), and the total social support was significantly higher than the control group in the posttest 1 (T = 2.137, P < 0.05).
Figure 1 shows that compared with pre-test, both of the total scores of G-CBT group and the control group reduced in the post-test 1 and then gradually stabilized. Figure 2 shows that compared with pre-test, the total scores of G-CBT group increased significantly in the post-test 1 and then gradually reduced in the post-test 2.
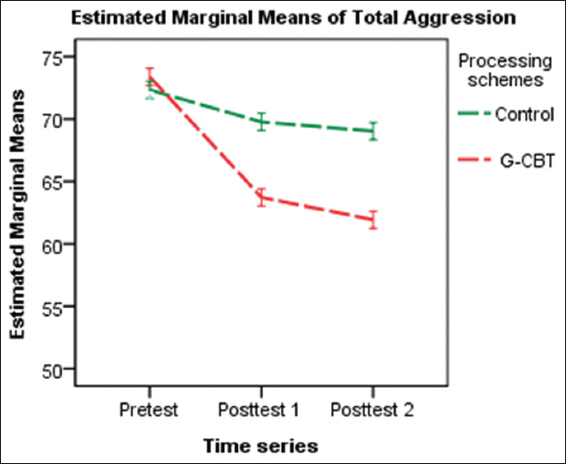
Figure 1: Plot of intervention effect for total aggression
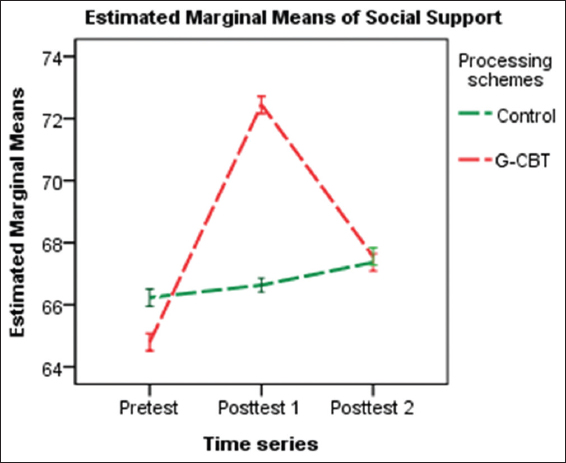
Figure 2: Plot of intervention effect for total score of social support
DISCUSSION
In the present study, the G-CBT included many links such as the choice of subjects, the therapist’s attitude, and the structure of group activities. Without careful planning and reasonable arrangement, these factors might disrupt or even destroy group therapy. The researcher thought seriously about these factors before the intervention and made the program of group activities combined with the characteristics of this study. First, the nature of the G-CBT groups was homogeneous, structured, developmental, and closed; second, the researcher had accepted the professional training and with practical experience; third, the researcher paid attention to abide by the following principles in the process of intervention: (1) To follow the principles of cooperation, guidance-finding, and Socratic learning; (2) to closely observe the relationship between group members, to encourage open and supportive feedback; (3) to implement the group activities in strict accordance with the established schedule; (4) to balance the group cohesion with empathy style; (5) to solve all kinds of obstacles and problems within the group; and (6) to provide enough autonomy and promote mutual cooperation between the members.[63]
In addition, the researcher gave full consideration on how to promote the subjects’ learning process, avoiding highly structured rote learning, also avoiding the unstructured and non-directive methods. In this study, the researcher found that in the process of intervention, there was at least one participant in almost every group who challenged other members or leader. To resolve conflicts triggered by challenging members and increase the cohesion of group was very important. Imperious type, for example, the participants tended to dominate the time of the groups, the researcher used the roundabout strategy or containment strategy to control. Besides, the researcher paid more attention to timely present educational materials in the interaction, to avoid the excessive sermon. In this study, there was only one participant who did not finish the post-test 1 and the post-test 2, and all the rest of the participants had finished the experiment and measurements. This would not influence the results basically.
For the control group, compared with pre-test, there was a significant change on the total score of aggression, the total score of aggression had dropped significantly (F = 3.594, P < 0.05). Through further analysis of the subscales scores, the result showed that the hostility factor had significant difference between pre-test, post-test 1, and post-test 2. Hostility score decreased significantly in the post-test and tracking (F = 3.813, P < 0.05). This mainly involved the internal validity of the design of experiment. Internal validity refers to the degree of a research study design, which correctly shows the results of the study, or causal relationship between independent variables and dependent variables. All factors which belong to the study design can be factors that affect internal validity. These factors mainly include the historical events, the subjects’ maturation, research tools or instruments, statistical regression, the selection of subjects, and the disappearance of the subjects and so on. In this study, all participants had just entered the universities. Compared with high school, the environment has changed. In addition, the survey found that all these three universities offer the course of College Students’ Mental Health for the 1st year of students. This may affect the results of the study to some extent. This study adopted the randomized pretest-posttest control group design, after the randomization balanced the conditions, the general history events which might have influence on the control group would also produce the similar effects on the G-IPT group. On the premise of subjects with homogeneity, and through a series of control measures, the researcher believed that the differences between processing schemes were caused by the independent variables.
According to the statistical analysis of G-CBT for aggression, there were significant differences on the total score and the scores of all subscales between pre-test, post-test 1, and post-test 2. For impulsivity, there was a significant difference between pre-test, post-test 1, and post-test 2 (F = 4.019, P < 0.05). Combined with the descriptive statistics, the score of impulsivity in the post-test 1 was slightly lower than the pre-test, but it reduced more obviously in the post-test 2. Impulsivity concerns a propensity of acting on a whim and behaves by little consideration or reflection of the aftermath that imperils long-term goals and strategies for success.[64] Impulsivity is both a trait of personality and a main component of many disorders such as borderline personality disorder, antisocial personality disorder, and aggression.[65,66] CBT for disorders involving impulsivity is common. As a relatively stable personality factors, it seems to be reasonable that the long-term effect is better than the short-term effect. For hostility, there was significant difference between pre-test, post-test 1, and post-test 2 (F = 4.726, P < 0.05). Combined with the descriptive statistics, the score of hostility in the post-test 1 was obviously lower than the pre-test, but it appeared a slight rebound in the post-test 2. Hostility is the state of bad feeling and ill will. It is seen as emotional and angry behavior and is often used as a synonym for aggression. The subjects of this study were first grade college students. Just entering the universities, they were not familiar with the environment and the people around them, so they were easy to produce hostility and wariness. As they were gradually familiar with the environment and the people around them, these emotional reactions including hostility might be reduced. This trend had been reflected in the control group. Coupled with the effect of intervention, the phenomenon of the obvious reduction of hostility could be understood. For physical aggression, there was significant difference between pre-test, post-test 1, and post-test 2 (F = 20.696, P < 0.01). Combined with the descriptive statistics, the score of physical aggression in the post-test 1 was obviously lower than the pre-test, and the score of physical aggression in the post-test 2 was basically the same as the after test. Physical aggression is behavior threatening or causing physical injury toward others that include biting, hitting, kicking, biting, using weapons, or damaging possessions.[67] This result was similar to other previous research results and proved once again that the G-CBT was effective for controlling physical aggression and the effect was stable. For anger proneness, there was significant difference between pre-test, post-test 1, and post-test 2 (F = 5.683, P < 0.01). Combined with the descriptive statistics, the score of anger proneness in the post-test 1 was obviously lower than the pre-test, and the score continued to decline after post-test 1 but tended to be slow. This further showed that G-CBT could quickly and effectively change the subjects’ anger proneness, and the intervention effect was durable. In general, the implementation of the G-CBT significantly reduced all subscales’ score, which further reduced the total score of aggression.
According to the statistical analysis, for the groups of G-CBT, there was no significant difference on the score total self-control between pre-test, post-test 1, and post-test 2 (F = 0.244, P > 0.5). In fact, recent evidences of behavioral genetics have shown that in terms of self-control, from 55% to 66% of changeability is descendible[68,69] and the stability still has a firm genetic basis over a long period.[70,71] This seemed to be an explanation as why the total score of self-control did not change significantly after intervention in this study. However, this did not mean that the processes of socialization were not significant in the progress of self-control. Actually, genetic factors predict aberrance in the interaction with environment,[72-74] just like shown in some other intervention studies.[75,76] If after a much longer period of self-regulation practice, the level of self-control might have further improvement.
According to the statistical analysis, there were significant differences on the total score (F = 5.743, P < 0.01) and the subscales of subjective support (F = 5.953, P < 0.05) and utilization degree (F = 6.616, P < 0.01) between pre-test, post-test 1, and post-test 2 for the participants of G-CBT. Combined with the descriptive statistics, the implementation of the G-CBT significantly increased the subjective support, utilization degree, and total score. There was no significant difference on the score of objective social support (F = 1.237, P > 0.05). This reminded that the level of subjective evaluation and feeling of social support had been improved. This change mainly came from the interpersonal problem-solving technique and social skill training. Based on this, the score of utilization degree had changed significantly after intervention. This proved that the participants were able to feel, evaluate, and utilize the social resources more reasonably. At the same time, the improvement level of social support could further help the subjects solve interpersonal problems and contradictions, ease pressure, and then reduce aggression.