INTRODUCTION
Estimates for number of suicides in India vary. For example, one study projected 187,000 suicides in India in 2010, while official data by the Government of India claim 134,600 suicides in 2010.[1] According to WHO data, the age standardized suicide rate in India is 16.4 per 100,000 for women (6th highest in the world) and 25.8 for men (ranking 22nd).[2] Reports from the World Health Organization (WHO) indicate that suicide accounts for the largest share of the intentional injury burden in the developed countries and that suicide is projected to become an even greater contributor to the global burden of disease over the coming decades.[3]
Serious suicide attempt (SSA) is a distinguishable phenomenon that needs to be addressed specifically within the scope of suicidal behavior. Interpersonal problems, as well as impulsivity and aggression, seem to facilitate SSA when mental pain serves as a secondary factor. Health-care professionals should be aware of SSA and familiar with its specific risk factors. Moreover, the role of suicide intent and planning in SSA is still unclear. Further studies should aim to clarify and refine the concepts and measures of SSA, thereby enabling more specific and concrete modeling of the psychological element in its formation.[4]
Suicidal behavior is a leading cause of injury and death worldwide. Suicidal behavior is any action that could cause a person to die, such as taking a drug overdose or crashing a car on purpose. Information about the epidemiology of such behavior is important for policy making and prevention. While the prevalence of lifetime suicidal behavior was found to be as 2.23%, the prevalence of lifetime suicide planning or attempt was 3.58%, suicide ideation for the past 1 year 1.43%, lifetime suicide attempt 1.43%, and lifetime suicide intention 0.62%. Suicidal behaviors were more frequent in involuntary marriages than involuntary ones. With the increased duration of marriage, both suicide behavior and suicide ideations were decreasing significantly. The rate of suicide ideation was significantly higher for individuals with alcohol abuse history than the ones without history of alcohol abuse.[5]
A postvention is an intervention conducted after a suicide, largely taking the form of support for the bereaved (family, friends, professionals, and peers). Family and friends of the suicide victim may be at increased risk of suicide themselves. The term “postvention” is a great example of suicide prevention jargon that means little to those outside the field and may actually contribute to misunderstanding. Postvention refers to activities which reduce risk and promote healing after a suicide death. Although postvention is implemented after a suicide, it is essential that we prepare for postvention before a suicide.[6]
There is now convincing empirical evidence that exposure to suicide increases the risk of subsequent suicide, as well as other negative mental health sequelae, in those who have been exposed. It also concludes that the substantial evidence base makes the case that all suicide prevention programs need to include postvention services as a direct form of suicide prevention.[7]
The survey generated three strategies for future postvention research, increases intercultural collaboration, increases theory-driven research, and builds bonds between research and practice. Future surveys should include experiences with obtaining research grants and ethical approval for postvention studies. Paucity of research literature on postvention for suicidal behavior initiated the investigator to conduct the present study. The novelty of the research work is on postvention for suicidal behavior among suicidal attempted clients.
MATERIALS AND METHODS
After obtaining written informed consent, suicidal-attempted clients who fulfilled the inclusion criteria such as with first suicide attempt, conscious, both gender, age between 20 and 60, common methods of suicide, who were able to give informed consent, and who understand Tamil were recruited and enrolled in the study on April 2018.
The design used for the present study was pre-experimental where one group pre-test–post-test design selected to determine the impact of postvention on suicidal behavior among suicide attempted clients. The total sample size was 40 suicide-attempted clients in Government Head Quarters Hospital at Erode. Purposive sampling technique was adopted in this study.
All participants were interviewed before intervention by assessing demographic and clinical variables such as age, education, occupation, work pattern, family monthly income, residence, and family history of suicide, blood group, and psychoactive substance use, respectively. The level of suicidal behavior was assessed by Osman Suicidal Behavior Questionnaire revised version. Immediately after pre-test, the participants received postvention treatment which comprises of one-to-one session. The session schedule was as follows:
-
Session I - Introduction
-
Session II - Psychological trauma
-
Session III - Suicide Communication Events
-
Session IV - Problems related to suicide
-
Session V - Follow-up.
Sessions I and II were administered during the 1st week, sessions III and IV administered during 2nd week and session V administered during 3rd week. Postvention treatment was given twice a week, for 3 consecutive weeks, with a duration of 30–45 min. The early 20–30 min spares to express psychological trauma, suicide communication events and problems related to suicide by the participants and subsequent 10–15 min for rendering psychological trauma therapy, suicidal communication strategies and problem solving strategies intervened by the investigator. The intervention was rendered for 2 weeks with follow up sessions during 3rd week onwards by using telephone mode. Post-test was conducted using the same assessment techniques after the follow-up session at the time of review. Pre- and post-test was conducted in-person.
The study was conducted after getting the approval from the Institutional Human Ethical Committee. Written permission was obtained from the chief medical officer, Government Head Quarters Hospital at Erode to conduct the study. Pilot study was executed to check the feasibility and time requirement of the study. Subject’s right to withdraw/withhold the information was ensured before data collection. After clarifying the doubts, signature was obtained from the suicide-attempted clients. Written informed consent was obtained from each participants related to the study purpose, type of data, nature of commitments, participations, and procedure. Oral consent was also obtained from the subjects for their willingness to participate in the study. Telephone contact information was obtained from the subjects who participated in the study. Risk benefit ratio was calculated. Confidentiality of the data was ensured throughout the study.
RESULTS AND DISCUSSION
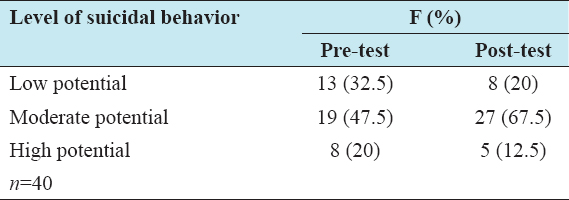
Pre-test showed 32.5% with low potential of suicidal behavior, 47.5% of the subjects had moderate potential of suicidal behavior, and 20% of the subjects had high potential of suicidal behavior. In post-test, 20% had low potential of suicidal behavior, 67.5% of the subjects had moderate potential of suicidal behavior, and 12.5% had high potential of suicidal behavior [Table 1].
Table 1: Frequency and percentage distribution of pre- and post-test scores on suicidal behavior
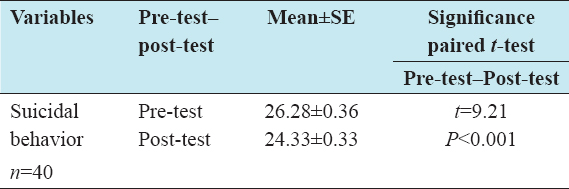
Comparison of mean and standard error of pre-test suicidal behavior scores showed 26.28 ± 0.36 and post-test showed 24.33 ± 0.33. The results were comparable to the significant difference between the mean pre- and post-test suicidal behavior scores. The mean score scaled down in course of post-test and showed significant decline of suicidal behavior among suicide-attempted clients. The Paired t-test value of suicidal behavior scores presented in Table 2 showed statistical significance (t = 9.21).
Table 2: Comparison of mean, standard error, and paired t-test value with pre- and post-test scores of suicidal behavior
Similar results were reported on postvention which assists survivors in grief and bereavement and attempts to prevent additional negative outcomes.[8] One of the researches reported that only few psychiatrists used suicide postvention procedure or toolkit (9%). No psychiatrists stopped the clinical practice after a patient suicide, although 10% stopped accepting patients they deemed at risk of suicide. Postvention efforts, therefore, should be improved to better address survivor care.[9]
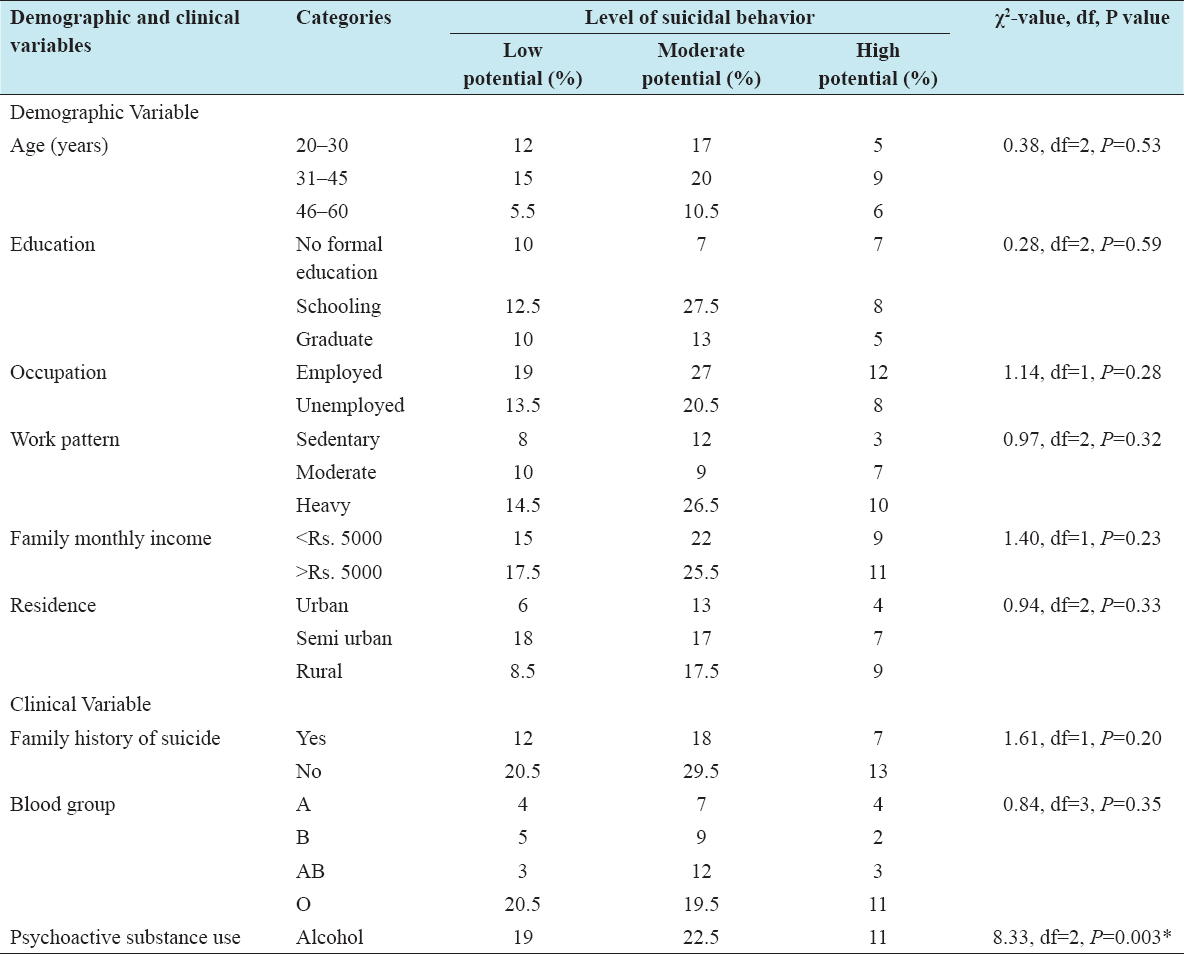
Association was found to be significant (χ2 = 8.33; significant) between pre-test suicidal behavior scores and the clinical variable of psychoactive substance use. No significant association was observed between pre-test suicidal behavior scores and clinical variables such as family history of suicide and blood type, whereas no significant association was observed between pre-test suicidal behavior scores with their selected demographic variables such as age, education, occupation, work pattern, family monthly income, and residence [Table 3].
Table 3: Association between pre-test suicidal behavior scores and the selected demographic and clinical variables
CONCLUSION
Based on the findings of the study, the following conclusions were drawn. The study findings revealed that administration of postvention was highly significant in the reduction of suicidal behavior among suicide-attempted clients. Henceforth, postvention could be depleted as an effective intervention strategy for prevention of further suicide, in suicide-attempted clients.