INTRODUCTION
Living a life without developing one of the numerous non-communicable diseases at any stage of life has become a major challenge women are facing today. Although most women are aware of the benefit of healthy lifestyle, yet majority of them find it difficult to change their unhealthy behavior capable of predisposing them to diseases. Worstill is women who are rural and semi-urban dwellers that are in the web of ignorance, scarcity, prejudice, and cultural taboo capable of influencing their health and lifestyle. Health is a state of complete physical, mental, and social well-being and not merely by the absence of disease or infirmity, while lifestyle is the way of life of a person or group of persons.[1] Healthy lifestyle helps to improve health and serve as a protector against diseases. Poor health results when a person or persons are unable to adopt the principle of healthy living such as good nutrition, access to clean environment, access to clean water, and access to good medical facilities.[2]
Literature has it that 80% of the premature heart disease stroke, type 2 diabetes and 40% of cancer could be prevented through the adoption of a healthy lifestyle.[3] It has become obvious that chronic diseases cannot be completely restricted despite the advances in science and technology without a change in lifestyle of the people. It is, therefore, important to monitor activities that predispose women to diseases all the way through investigations to provide the required assistance.
Most custom and traditional practices in Nigeria expose women to health and other challenges than other members of their household. Culture in Ojua et al.[4] is that complex whole which includes knowledge, belief, art, morals, laws, customs, and any other capabilities and habits acquired by man as a member of the society. Culture in its simplest type can be said to be the mode of life of inhabitants of a community. The people firmly hold fast to the dictates of their cultural values given that they stand to get punished or undergo some misfortunes if they break the rules or laws of their culture. These practices not only impinge on their health but also other aspects of life as well as communal interaction and disease conditions. Some are advantageous while others are among the harmful cultural practices include female genital mutilation, child marriage, various taboos, or practices which stop women from controlling their productiveness: Dietary taboos such that prohibit them from eating some nutritious foods, traditional birth practices, son preferences, female infanticide, and dowry price to mention but a few.
Nutritional taboo or food taboo is a purposeful averting of nutritious food for reasons other than detest from food preference. Food taboo has been identified as one of the contributing factors to maternal undernutrition in pregnancy.[5] In some customs and traditional practices, expectant and lactating mothers are required to refrain from nutritious foods advantageous to their health. The custodian of the traditions of the land makes out certain foods as forbidden giving different reasons which in most cases are not true. In all of these, the significance of food to the general health of women cannot be overemphasized, knowing that malnutrition is a life series syndrome, which results to greater diseases later in life such as obesity, diabetes, and cardiovascular diseases. Women and younger children have been known to bear the burden of malnutrition in the rural setting and one of the reasons being nutritional taboos practiced by the people.[6,7]
The dietary status of women is predominantly significant since it is through women that their offspring emanates. An underfed mother is prone to giving birth to a low weight baby that will be vulnerable to diseases and untimely death. An aspect of undernourishment largely suffered by women is undernutrition, which is a major cause of ill health and casualty among women. Food taboo which is one of the taboos represents unrecorded communal rules mainly based on sacred cultural/chronological reasons that control the food accepted in a community. Food taboo and beliefs lie with the contextual factors included as one of the basic causes of malnutrition.[8] In line with the undernourishment saddle suffered by women and children around the world, the United Nations advocate nutrition interventions during the critical 1000-day window which is to take care of mother and child’s critical period of life.
In Esan West Local Government Area, food taboo is very much experienced under Ishan tradition and laws, like most Nigeria customs, customary practices are stuffed with laws and taboos aimed at perpetuating tradition. This has influence on the lifecycle of the woman in an attempt to obey the laws and custom of the land. For instance, women that are pregnant are prevented from eating milk, eggs, and snail. Gizzard and thighs of chicken or ducks are eaten by the men or elderly. Young mothers in some part of Benin and Ishan must not eat fresh meat or oil soup for days after postpartum. Investigation on nutritional taboo practices has been carried out in most ethnic groups in Nigeria.[4,9] None has been recorded in Esan West Local Government Area of Edo state. In light of all these, this study was, therefore, undertaken to determine the healthy lifestyle and nutritional taboo practices of mothers in Esan West Local Government of Edo state of Nigeria.
LITERATURE REVIEW
Healthy Lifestyle
Healthy lifestyle practices are viewed by Chung[10] as a multidimensional pattern of self-initiated actions and perceptions that serve to maintain or enhance the level of wellness, self-actualization, and fulfillment of the individual.[11,12] Enumerated the following as behaviors which influence personal health as individual nutrition, physical activity, stress management, psychological wellness, health responsibility, not smoking, having little or no alcohol, having breakfast, not eating junk food, keeping an ideal body weight, sleeping for 7–8 h a day, and having adequate exercise. While[13] Pender indicated the determining factor of healthy lifestyle as cognitive perceptive factor such as the realization of the importance of health, other studies such as[14] perceived social economic status, level of education, family, kin, and social networks, gender, age, and interpersonal influences as the determining factor. In the predictor of healthy lifestyle, findings from the studies of Wange and Liu[15] pointed to presence of chronic diseases, higher educational level, and better socioeconomic status were found to have greater abilities of living healthy lifestyle.
NUTRITIONAL TABOO
Nutritional taboo is as universal as food. It is commonly practiced. For instance, Ezema and Ezema[16] assessed attitude and sociocultural practice during pregnancy among women in Oyo state, it was found that cultural beliefs played significant roles in determining the kind of food women consume. A study by Alli et al.[17] in Pakistan showed that 12% of adult women in a community health center in Pakistan believed in restricting some food items during pregnancy. Some of these traditional practices, especially food taboos, are known to contribute significantly to maternal malnutrition, Kuzma et al.[18] also reported same among pregnant women in South Eastern Nigeria and Papua New Guinea, respectively.
Purpose of the Study
The purpose of the study was to examine the healthy lifestyle and nutritional taboo practices among rural women in Esan West Local Government Area of Edo state. Specifically, this study determined the following:
-
The demographic characteristics of the mothers attending the health center
-
The healthy lifestyle practices by the women attending the health center
-
The nutritional taboo practices by women attending the health center.
METHODOLOGY
This study was conducted in Esan West Local Government Area of Edo state, using a survey research design. 300 mothers that were attending the primary health-care center of the local government area constituted the study. Simple random sampling technique was adopted to select from 700 mothers that attended the center within the study period. Every second mother attended at the clinic was included in the study.
Instrument for Data Collection
A semi-structured interviewer-administered questionnaire captioned healthy lifestyle and nutritional taboo practices by mothers questionnaire was utilized to collect data for the study. The instrument had three sections: Section A was used to obtain information on their sociodemographic characteristics such as age, level of education, household size, main occupation, and marital status while Section B was designed to measure the healthy lifestyle practices and Section C sourced information on nutritional taboo practices by the respondents.
Data Analysis
The data collected were analyzed using descriptive statistics which are frequency counts and percentages.
Ethical Consideration
Approval for the research was obtained from the Local Government Area Council (Health Department) in the LGA before the research and also an up to date consent was obtained from each respondent before the questionnaire was administered.
RESULTS
Table 1 shows that respondents were in their energetic years 25–40, 127 (42.3%) and 40–50, 109 (36.3%). The finding also indicate that the level of education respondents are as follows; No formal education 59(19.69%), Primary education, 151(50.3%), and Secondary education 79(26.3%), National Diploma 09(3%), HND/B Sc2(0.66%) respectively. The household size of the respondent is between 5 and 7, 181 (60%).Majority of the respondent’s household size were between 5 and 7, 181(60%) while the respondent’s main occupation were; Trading 125(41.67%), Farming 125(41.67%).
Table 1: Demographic information of respondents
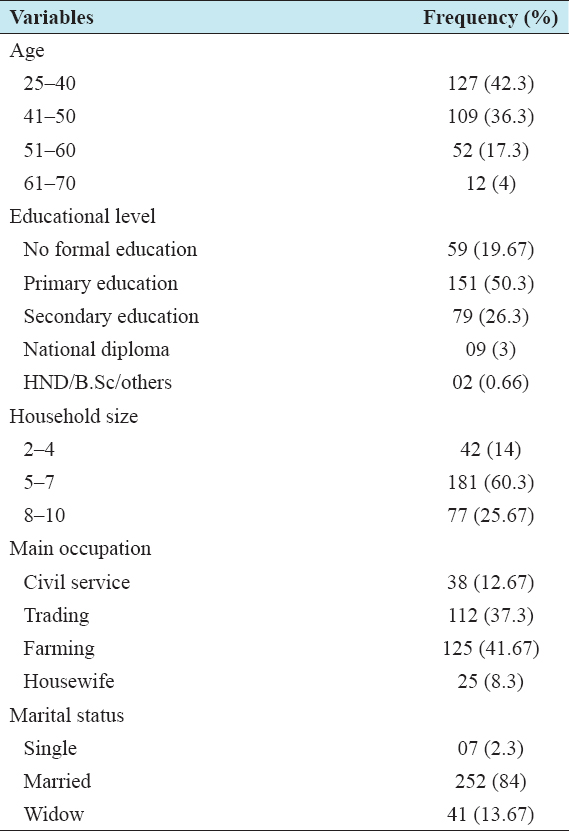
Table 2 indicates that a low proportion of mothers visit hospital regularly for medical checkup 32 (10.7%) and most of the rural women do not visit hospital regularly 268 (89.3%). None of the women smoke or take tobacco 300 (100%). Higher proportion of the women is exposed to smoke 268 (89.3%) while 32 (10.7%) were not exposed to smoke. Most of the respondents do not have regular water supply or clean water 298 (99.3%). Majority of the respondents 202 (67.3%) believe in the use of herbs in the treatment of disease 202 (67.3%). High proportion of respondents 181 (60.3%) prefer to be delivered by traditional birth attendant while 119 (39.7%) prefer orthodox practices. Majority of the respondents skip meals 202 (67.3%) while 88 (29.3%) do not skip meals. Furthermore, 187 (62.3%) still believe in circumcision while 113 (37.7%) do not believe that female should be circumcised. Those that visit neighbors are more than those that do not socialize 244 (81.3%)–56 (18.7%).
Table 2: Research Question 2: Healthy lifestyle practices of respondents
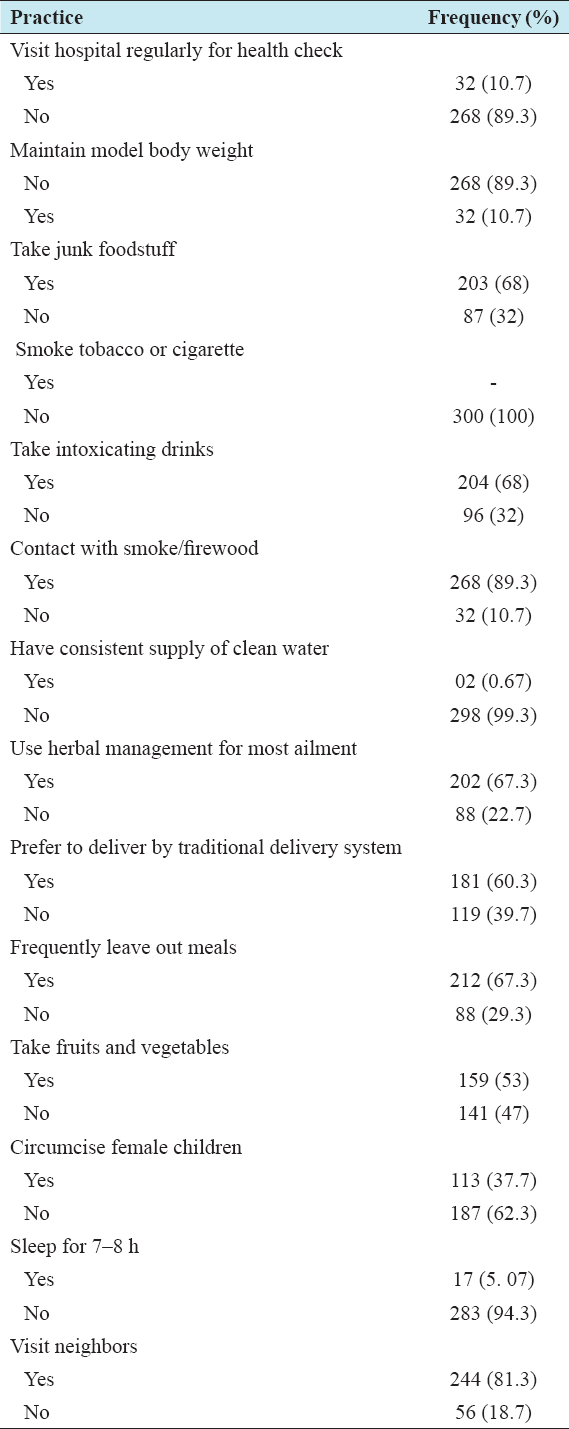
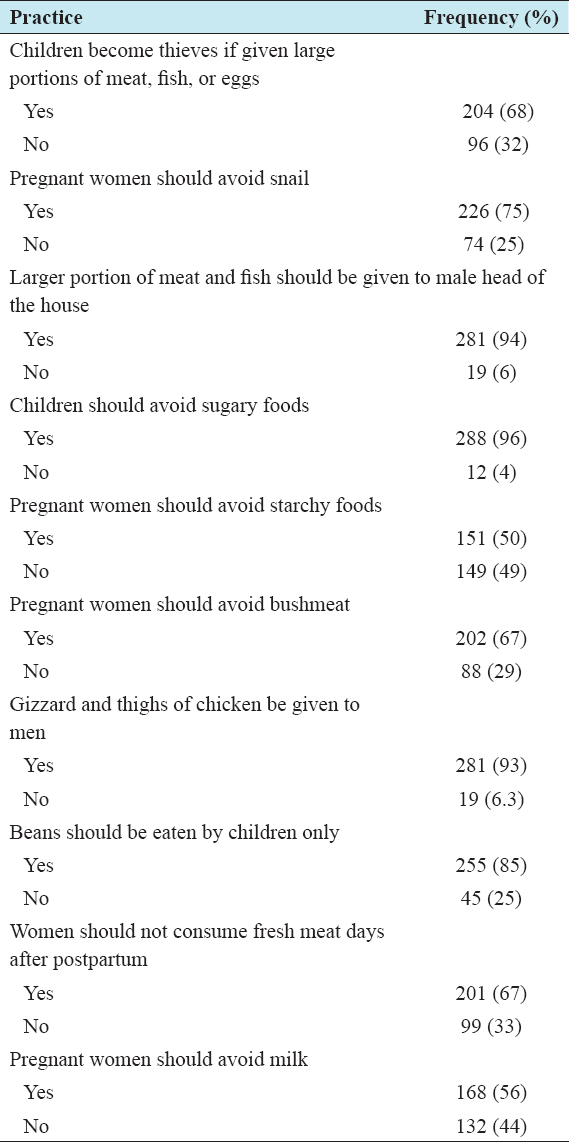
Table 3 indicates the food taboo practiced by the respondents are as follows that children would become thieves if given large portion of meat, fish, or eggs (68%), pregnant women should avoid snail (75%), larger portion of meat should be given to the man in the house (94%), children should be made to avoid bushmeat and certain meats (72.2%), gizzard and thighs of chicken should be given to the men (89.7%), and women should not consume fresh meat days after postpartum (67%).
Table 3: Nutritional taboos practices of respondents
DISCUSSION
The results in Table 1 showed that majority of the respondents were between 25 and 40 years indicating that they were in their energetic years. This finding is supported by FAO[19] which reported that women of such category are in their active and vitality age for they are in their childbearing period. It is expected that they should be present at the clinics for prenatal and postnatal visits. Educational level of the respondents also showed that majority of the respondents have primary school leaving certificate. Education helps an individual to change his or her behavior without being forced. The household size of the respondent is between 5 and 7, 81 (60%). This implies that most of their households are already tending toward a large sized family.
A lifestyle is healthy if it is accompanied with good practices such as regular visit to the hospital for medical checkup; result from the study is contrarily to the ideal practice. These women do not visit hospital. This is finding is further strengthened by Okechukwu[21] who reported that the number of women that utilize health-care facilities is still low, even when they have health challenges. This is injurious to their health; therefore, it has to change. Similarly, findings from this study indicate alcohol usage among the respondents, this corroborates report of Abor[22] that declared that regular smoking and high level of alcohol consumption in the adult population of his research; however, this observation may not be a general practice among adults as observed from the work of Fadupin[23] who found a low incidence of alcohol consumption among school teachers. This discrepancy may be credited to standard of living differences in environmental regions and cultural groups in Nigeria. Alcohol is one of the most commonly used psychoactive remedies in Nigeria. In addition, studies in Nigeria have connected alcohol addiction and extreme alcohol use with foremost health chaos among young adults and a strong risk factor for stroke in adults >45 years.[23]
Findings from Table 3 revealed that the nutritional taboo majorly practiced is as follows that children would become thieves if given meat, fish, or eggs, pregnant women should avoid snail, bushmeat, and certain meats, gizzard and thighs of chicken should be given to the men. This finding is supported by Adekunle and Unuorah[7] who reported that food taboo is still been practiced among the rural dweller, in many local government areas in Nigeria, several households do not eat certain meats because they were rejected animals. The children were deprived of eating these foods until they are matured lest they steal. According to him, the habit of serving better parts of animals and animal protein for male elders at the expense of the children is a common practice even among the enlightened families. In Esan West, many households have fixed ideas about what they eat and generally relied on staple foods such as cassava, yam, and like as first infant foods. Such parents confine their family from eating rats, snails, and gizzards even when they were unable to get enough protein. The nutritional taboos and restrictions consequently benefited the adult males at the cost of the susceptible groups that have fairly larger dietary requirements. In most cases, the affected foods are of animals’ source which is in a very short supply. These dietary taboos in most cases limit the intakes of vital nutrients among the people that practice them.
CONCLUSION
Women’s health and nutritional well-being are of paramount significance to the development of any nation. A hale and hearty woman nurtures a strong family and a healthy family makes up a healthy nation. The lifestyle and nutritional taboos of mothers studied so far revealed the unhealthy lifestyle practices and nutritional taboo practices capable of predisposing mothers to non-communicable diseases; therefore, there is a need for women to be in charge of their own health and welfare. They must do by shifting from their old lifestyle to meet the expected health standard. Furthermore, women have to acquire knowledge by taking advantage of government adult literacy programs in their local government areas so as to decrease the prevalence of maternal malnutrition.
Implication for Nutrition Education
The finding of this study points to the fact that women are still dwelling in ignorance even in the 21st century when information is at its climax; therefore, urgent intercession in the area of nutrition education is needed. This is important to raise the health of young women of reproductive age in the state. In addition, foodstuff supplementation programs should be enhanced to target young mothers and undernourishment among children. Nutrition education should be made to aim at improving women nutrition behavior. There should be ways of teaching behavioral changes in vital areas such as food choice and food taboo. Besides, pregnant women should be well educated on the importance of taking their regular folic acid and multivitamin supplements for encouraging pregnancy outcomes.
Recommendation
Based on the findings, the following recommendations were proffered that:
-
Efforts must be intensified in the area of nutrition education with emphasis on lifestyle modification.
-
Statewide categorization of nutritional taboos should be undertaken to support the effort of the health sector in the area of nutrition education.
-
Government should make available wide move toward nutrition education by including nutrition into the primary school curriculum.
-
Women education should be encouraged by the government to eliminate ignorance among women.