INTRODUCTION
Water supply and sanitation are two essential sectors to build up a development plan in an area. In specific, access to water supply and sanitation is basic human needs and rights. Worldwide, 71% of the rural population has access to improved water supply and 38% has access to improved sanitation.[1] Bangladesh has been facing multiple challenges in the sanitation, hygiene, and water sectors since its foundation day (December 16, 1971 - victory day). In accordance with the Joint Monitoring Report of the WHO and UNICEF, latrine coverage stood at 56% in 2012 and the proportion of the population with access to safe water was about 81%.[1,2] Safe water and sanitation contribute to enhance the quality of life through improved general health conditions and well-being of the people. Safe water, sanitation, and hygiene promotion combined with a culture of safety toward natural disaster are critical to human and economic development. Bangladesh is one of the poorest countries in the world with water and sanitation-associated diseases that are the major cause of mortality and morbidity although surface water is abundant. The southwest coastal regions of Bangladesh have been experiencing an acute shortage of safe drinking water and increase in salinity intrusion in surface and groundwater over the past few years.[3] In general, the coastal region of Bangladesh is directly affected by high tidal surges, cyclone, and man-made cause. As a result, water source and sanitation facilities are damaged drastically. In addition, tube wells are either broken or partially damaged and become unusable due to submergence at aforementioned regions. Moreover, ponds and other water bodies are all contaminated by the onrush of saline water, thereby leading to a crisis of drinking water. As a result, the outbreak of waterborne diseases such as skin diseases, diarrhea, fever, and dysentery in the affected areas claims premature death of numerous human lives. Damage to sanitation facilities and infrastructures is also very alarming in all the worst affected area, and it can also occur from lack of knowledge and awareness.[4] Field experiences and studies suggest that a minimum quantity of safe water is required for a person to drink, prepare food, ensure personal cleanness, and use a sanitary latrine. In general, a person who practices personal hygiene and uses a latrine needs an absolute minimum of 120 L/day, but the people of the study areas are very unconscious about using water and sanitary latrine and they give a very little importance about on this issue. In the present world, water supply and proper sanitation are the most important challenging issue for all, and they are starting to work for solving this problem. At the beginning of 2000, one-sixth (1.1 billion people) of the global population did not have access to improved water supply and two-fifths (2.4 billion people) did not have access to improve sanitation, and the majority of these people live in Asia and Africa.[5] Bangladesh is a low-lying country in South Asia at the head of the Bay of Bengal, and most of the coastal regions are inundated with high saline water that is not possible to drink and use in other sanitation purpose. Due to salinity and lower standard, sanitation is the main cause of diseases, destroyed all infrastructures, and polluted the total environment. The national baseline survey of 1993 indicates that the rural coverage of households’ toilets is 87.5% and that only 7.5% of these could be considered sanitary. According to the statistical data in 2001, the proportion of households with sanitary toilets is 44.8% increase in rural area.[6] Water supply and sanitation in Bangladesh are characterized by a number of achievements and challenges. Around 5.1 million poorest people at coastal regions will get access to safe water, 1.5 million school children will achieve safe water and improved sanitation, and 4.5 million children will receive hygiene education in Bangladesh by 2021.[7-10] Bangladesh aims to achieve “Sanitation for all by 2030” and the government is investing a lot of money into achieving this goal. While the country has improved with increasing access to water supply and sanitation, about 28% of the urban population and 41% of the rural population still do not have access to safe water.[7-9] In contrast, only 74% of the urban areas and 57% of rural areas are covered with improved sanitation. According to Miguel et al., lack of sanitation and poor hygiene is responsible for the transmission of dysentery, diarrhea, cholera, malaria, typhoid, and several parasitic infections.[11] Most of the waterborne diseases such as roundworm, whipworm, guinea worm, and schistosomiasis are linked to poor sanitation, which are highest among the poor people, especially in school-aged children. These diseases have a strong negative impact on the health and nutrition of children and their learning capacities and contribute to significant absences from school.[12-17] More than 2.2 million people in developing countries, mostly children, they die each year from diseases associated with lack of access to safe drinking water, inadequate sanitation, and poor hygiene and unawareness. In developing countries, water is crucial for sustainable development and poverty alleviation. In 2002, 18% of the world’s population lacked access to safe drinking water, while 40% of the world’s population lacked access to improved sanitation services. At the Millennium Summit in 2000, Heads of state pledged to halve the proportion of people who are unable to reach or to afford safe drinking water by the year 2015.[13-16] This “Millennium Development Goal” (MDG) was reinforced by a similar goal for sanitation contained in the Johannesburg Plan of Implementation agreed to at the World Summit for Sustainable Development in 2002. The technological options in the rural water supply are shallow tube wells, deep tube wells, Tara tube wells, pond sand filters, rainwater harvesters, ring wells, and infiltration galleries depending on natural water quality and hydrogeological conditions.[7-18] There are several surface water treatment plants and sanitation systems such as pit latrine, ring slab, and so on which are applied to solve the problem by the government and different non-governmental organizations (NGOs).[6-10] The community-led total sanitation concept is a new approach to improve the sanitation coverage in rural areas that have been first introduced in Bangladesh and significantly contribute to the increase in sanitation coverage since 2000.[6-15]
This paper assesses safe water supply and sanitation facilities at Sholadana Union in Paikgacha Upazila of the coastal region of Bangladesh with the identification of major problems about safe water supply and sanitation facilities and exposes the community demand for the development of water supply and sanitation systems for a standard living.
METHODOLOGY
At first, the topic of the study has been conceptualized, and then, the objectives followed by the study area have been selected. After that, the data collection procedure follows, which involves questionnaire preparation with the help of the literature review and consultation with the supervisor, sample number selection with the same procedure; and then, the primary data have been collected through a household survey and the secondary data have been collected through some secondary sources (Internet, Bangladesh Bureau of Statistics, published and unpublished sources).[6-15] The collected data have been analyzed through some statistical software (Microsoft Office Word, MS Excel, and so on). Processed data have been analyzed in the feasible, simple configuration. The analysis is statistical and calculative as far as possible for the rationale of the study.
Field Survey Design
The study was undertaken with a view to identify the environmental conditions such as water supply, sanitation facilities, and health status of the affected coastal region of the existing situation. To achieve the objectives of household surveys, field visits and a questionnaire survey were conducted. “Household head” means the person who plays the main role in the decision-making process of a family. In the absence of the household head, the second important adult member of the family was interviewed. Information was also collected through “non-participatory observation.”
Features of the Study Area
Paikgacha Upazila is the southwest part of Khulna district. The Upazila occupies an area of 411.19 km2, and it is located between 22º28’ and 22º43’ north latitudes and between 89º14’ and 89º’28’ east longitudes shown in Figure 1. The study area Sholadana union is situated under Paikgacha Upazila and occupies an area of about 12085 acres as shown in Figure 2. Its total population is 23204 (male 12021 and female 11183) and the literacy rate is 46.85%.[6,10] The area, which has been selected for this study purpose, is only one small village (Nuniapara) of Sholadana union.
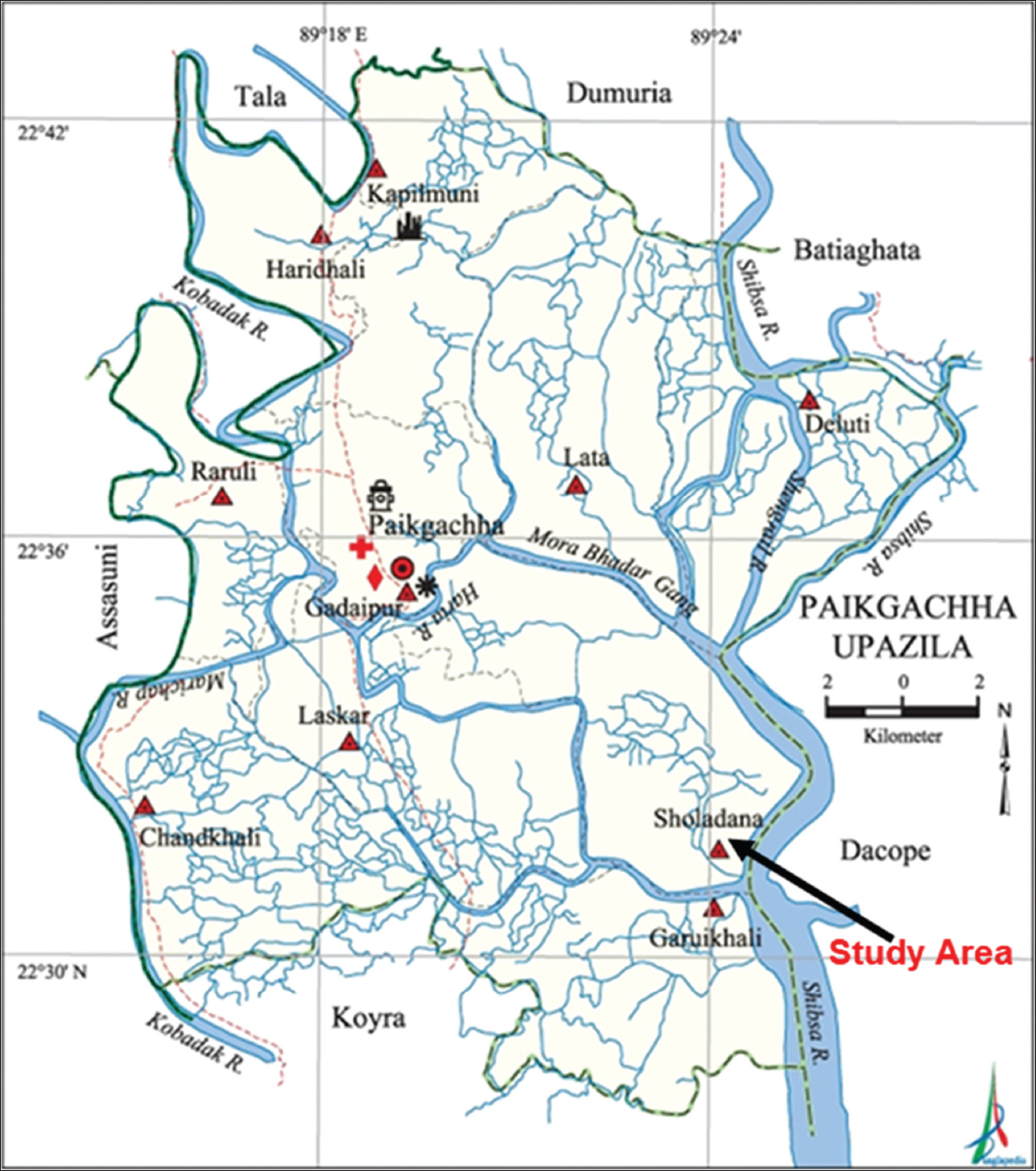
Figure 1: Map of Paikgacha Upazila in which Sholadana union is directed (Banglapedia, 2012)
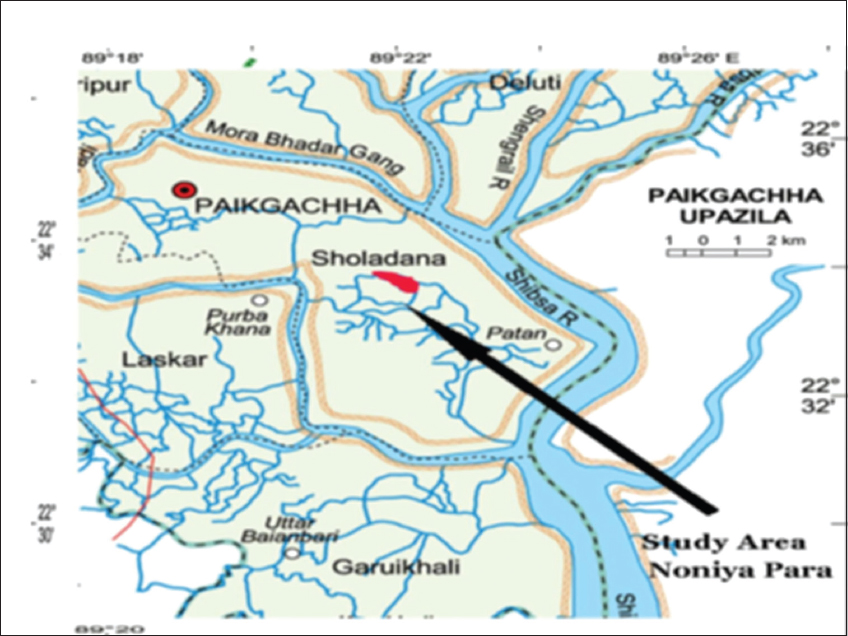
Figure 2: Map of Sholadana union in which studied villages are directed. (Source: Banglapedia, 2012)
For the study, field visits and a questionnaire survey were conducted in Nuniapara village under Paikgacha upazila in Khulna district in June–December, 2013. It is basically an acute saline prone area, and seawater intrusion is the causes of salinity by man-made and sometimes natural calamities. This area is popular for shrimp culture mainly for its high salinity and the total water, sanitation, and health condition are contaminated by salinity. The map of Paikgacha Upazila is shown in Figure 1 that has depicted the study area with respect to Bangladesh as well as with respect to Khulna district.
Justification of the Study
Usually, southwest coastal region has a crisis of safe drinking water, and natural calamities with tidal surge have affected water supply and sanitation facilities seriously in the coastal region of the country. As these areas are saline zone, so the usual source of water supply has fully disrupted due to inundation by saline water. In Nuniapara (Sholadana Union, Paikgacha Upazila, Bangladesh), the latrine standards are very low quality and poor condition. Different components of latrines including ring, slab, and water seal have been damaged due to poor quality components. The selected area has already been affected through diarrhea and other waterborne disease outbreak. Therefore, this study has been carried out to identify the key points related to the severe crisis of safe water, unhygienic condition of sanitation, and health risk to obtain viable solutions.
Objectives of the Study
The primary objective of the study is to investigate the overall ongoing situation of water supply and sanitation system in the coastal regions of Bangladesh and how they have to suffer in the adverse conditions. The specific objectives are as follows:
-
To identify the main causes related to poor water supply and sanitation system.
-
To count the different sanitation system in the study area.
-
To identify water and sanitation-related diseases and their consequences to public health.
Expected Outcomes
The possible outcomes of the conducted study are as follows:
-
The study will help to know the present status of water supply and sanitation system in the study area.
-
The study will reveal the effect of salinity and other harmful pathogen on human being and their total environment.
-
The study will establish an internal relationship among water supply, sanitation, and health status to explore possible solutions for the arise problems.
RESULTS AND DISCUSSION
In Bangladesh, more than three-quarters of total population (over 115 million) live in rural areas.[2-10] In general, rural people are very unconscious about water supply source and sanitation system. Among the poorest families, about one in three people defecates in the open. Of all the latrines in rural areas, only 32% meet the international standards for a sanitary latrine in that way they completely isolate excreta from the human environment through the use of a water seal U-bend or some other lid or barrier.[6,16] In rural areas where pipeline water supply system is yet undeveloped, people have to go around two or three kilometers to collect potable water. In most cases around 96%, women and children are involved in this job.[3,4,7-10]
In the early stages of epidemics such as diarrhoea and severe skin diseases were very common scenes in these areas due to salinity, which can be also responsible for lack of minimum health knowledge among the people. It was quite impossible for these bodies (government and NGOs) to provide such people with preventive measures such as creating awareness about salinity, waterborne diseases, the creation of safe water, and hygienic sanitation habit which are almost necessary for safe living. However, nowadays, the transport system in this area is available and the problem has gone off. For eradicating such a critical problem, we have to remove social backwardness and superstitions and to adopt new technology to solve the problem in the study area.
Socioeconomic Condition
Educational status of the respondents
The education status of the respondents in the carried study area is grouped into illiterate (30%), primary (32.5%), secondary (30%), HSC (2.5%), and graduate (5%). Illiterate means the person who does not have reading and writing skills, but they can do signature only. Thus, from the study, it was found that many people start their education from primary level, but very few people finish their education at a higher level.
Major Occupational Trend
There are various occupations of people in Nuniapara under Sholadana Union (Bangladesh) that includes farmer, fish cultivation, business, day labor, driver, and teacher. The occupational status of people in Nuniapara is farmer 0%, fish cultivation 27.5%, business 30%, day labor 32.5%, driver 7.5%, and teacher 2.5% as shown in Figure 3.[3-10] However, most of the people were involved with fishing in a previous time. According to the conducted field survey, the main occupation among residents was day labour (32.5%) at the then time and also most of the day laborers are related with fish cultivation activities. Hence, they are adopted with different occupations depending on their socioeconomic condition.
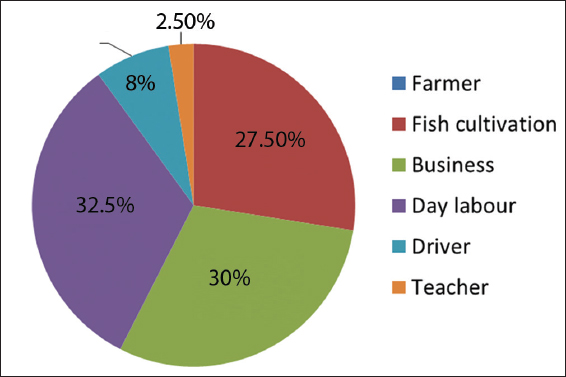
Figure 3: Major occupational trend in Nuniapara, Bangladesh
Income of the Household
It has been observed that about 25% people earn 3000–4000 BDT, 30% earn within 5000–6000 BDT, 20% earn within 6000–10,000 BDT, and 25% of them earn above 10,000 BDT (1 USD =79 BDT) as shown in Figure 4.
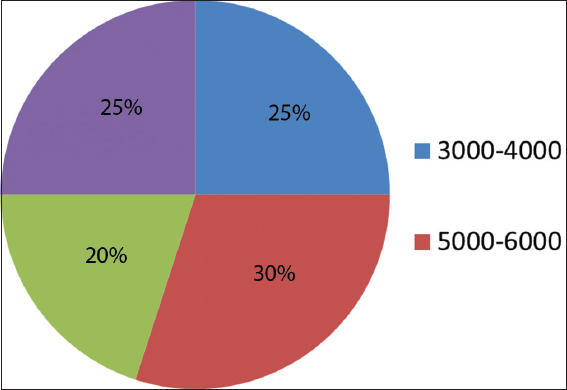
Figure 4: Income of the household/month in Nuniapara, Bangladesh
Settlement Condition
The housing condition is one kind of indicator of economic status. Figure 5 shows the housing condition in the study area which is grouped into two kinds, such as building and slum structure (Cacha Bari). Most of the house in the study area is slum structure. It indicates that 27.5% households are building and 72.5% households are slum structure. Hence, their settlement conditions are lower standard according to the WHO, UNICEF, and other NGO.
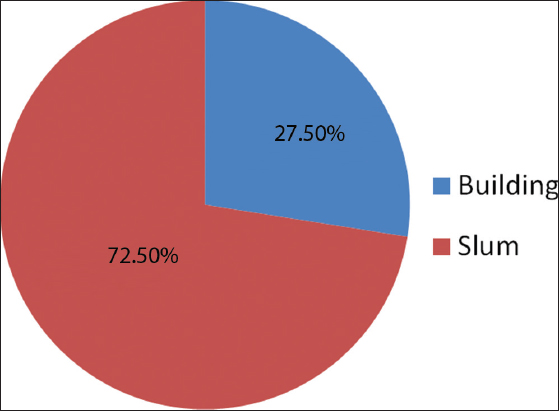
Figure 5: Settlement condition in Nuniapara, Bangladesh
Water Supply
The coastal region of Bangladesh is identified as a saline prone area because of seawater intrusion where complex hydrological situation makes more problem in drinking water supply system compared to other parts of the country. The environment of the coastal region is characterized as excessive salinity in both ground and surface waters resulting in poor coverage in the coastal belt.
Causes of Saline Water
From the field survey, it has been found that about 100% seawater intrusion is the main cause of saline water and the salinity remains from January to June in a year in the study area. However, another 6 months have low salinity in water in the study area because the salinity is diluted with rainwater. On the other hand, man-made cause is also responsible for water salinity by shrimp cultivation.[7-10]
Main Problem due to Saline Water
Salinity is the main problem in the study area, and due to saline water, drinking water scarcity, unhygienic sanitation, and health disease are occurring drastically. In addition, arsenic in water is one of the major problems in the study area. It has been also found from the survey [Figure 6] that drinking water scarcity is 72.5%, unhygienic sanitation is 10%, and health disease is 17.5% in the study area due to saline water. Hence, safe drinking water scarcity is the main problem for standard living in the study area.
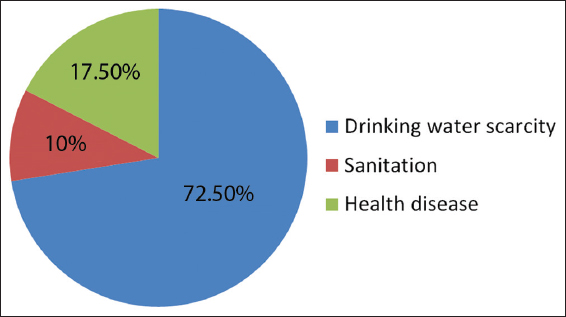
Figure 6: Different occurred problems due to saline water
Sources of Drinking Water
People of the existing community use different sources of drinking water such as rainwater, shallow tube well water, and purchasing water. It has been seen that 82.5% of the households use rainwater and shallow tube well water and 17.5% of the households use rainwater and purchasing water as shown in Figure 7. Hence, rainwater harvesting and shallow tube well water are the main drinking water source in the study area. Therefore, these sources are the only easy solution to fill up the demand of drinking water according to respondents in the study area.[5-9]
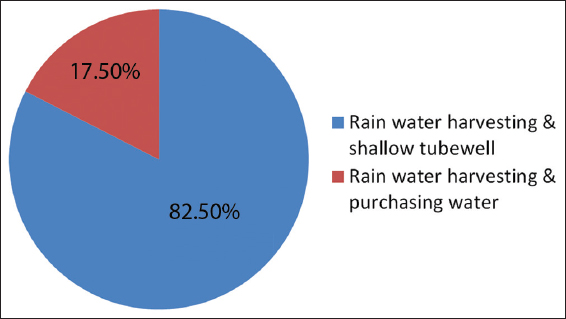
Figure 7: Sources of drinking water in the study area
Rainwater Conservation
Rainwater is an important source of drinking water in coastal part of Bangladesh. During the rainy season, all coastal people reserve the rainwater in drum, and some of the people drink this water in the whole rainy season and remaining of the people drink this water throughout the year. From the field survey, it has been observed that 100% households conserve rainwater during the rainy season and it is the only easy solution in the saline prone area to use safe water.[3-10]
Duration of Rainwater Using
From the field observations, it has been noticed that 12.5% households use rainwater for about 2–3 months, 15% households use for about 3–4 months, 57.5% households use this water for about 5–6 months, 12.5% households use for 8 months, and 2.5% households use more than 8 months [Figure 8].[3,4,7-10]
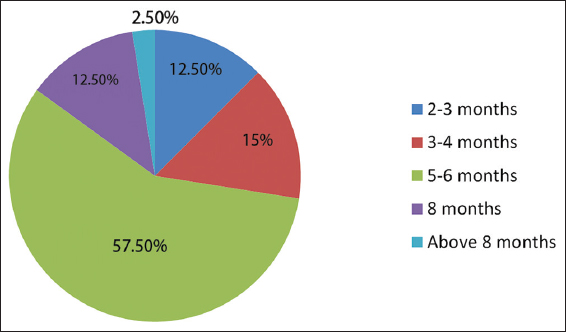
Figure 8: Duration of rainwater using in the study area
Method of Rain Water Harvesting
Rainwater harvesting is the most usable water conserving method in the present world for poor people, so it is also used to conserve water in the study area by different methods such as pitcher system, house system, and drum/tank system as shown in Figure 9. It has been observed that 37.5% households use pitcher system, 7.5% households use house system, and 55% households use drum/tank system to store water for drinking purposes in the study area, respectively. Here, drum/tank system is the highly used system for rainwater harvesting method as shown in Figure 10.
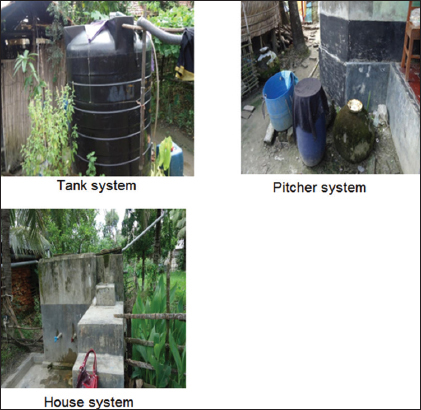
Figure 9: Different methods of rainwater harvesting
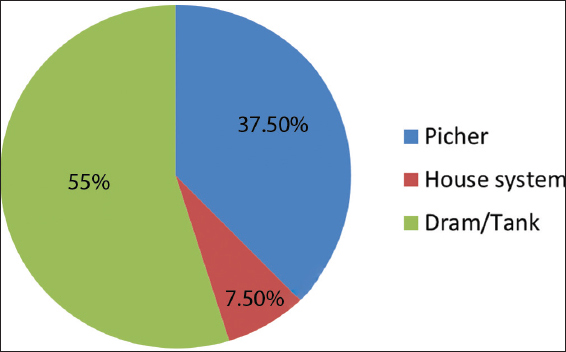
Figure 10: Percentage of different rainwater harvesting methods
Positive Side of Rainwater Harvesting
Rainwater harvesting is an easy process to collect water, and it can fulfil the demand of fresh drinking water without extra cost. From the field survey, it has been also observed that 100% households prefer to store the water using rainwater harvesting system.
Negative Side of Rainwater Harvesting
Rainwater harvesting is an important water reservation process in the coastal region because it is the alternative process for getting pure water in the saline prone area, but it has some negative sides during rainwater harvesting that includes pipe/pot leak, require to clean after few days and sometimes harvesting system can be failed. The negative aspects of rainwater harvesting system are shown in Figure 11.
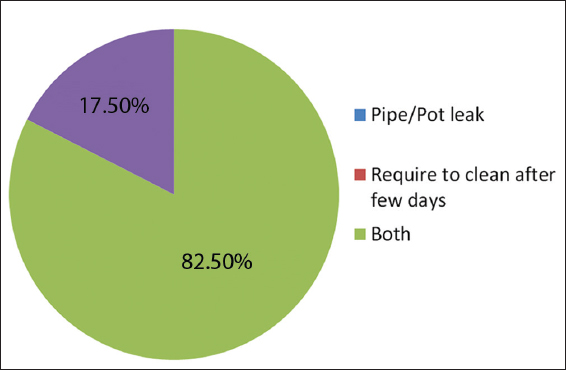
Figure 11: Negative side of rainwater harvesting
Extent of Purchasing Water
Percentage of purchasing water
Purchasing of water is very difficult to people in the study area because their economic condition is very low standard. Most of the households are not capable to purchase water because of their very low income and other household expenses. Only 22.5% households can purchase water, and around 77.5% households cannot afford to purchase water because of their lower socioeconomic condition as shown in Figure 12.
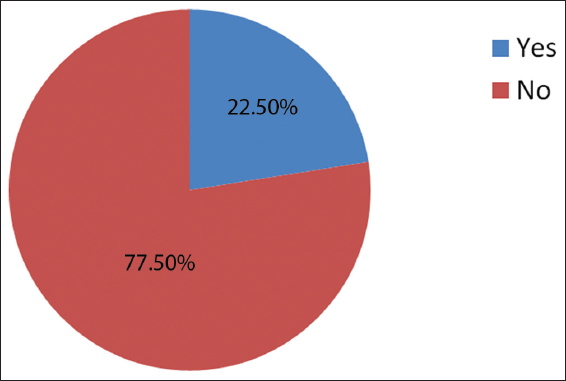
Figure 12: Percentage of local people use purchasing water
Duration of Purchasing Water
The study area is seriously affected by salinity, so they have to sometimes purchase water in the year when lack of rainwater, but some people use then shallow tube well water for the shortage of money. Figure 13 shows that 2.5% households purchase water for 2–3 months, 17.5% households purchase water for 3–4 months, 2.5% household use purchase water for 5–6 months, and 77.5% household do not purchase water in the whole year.
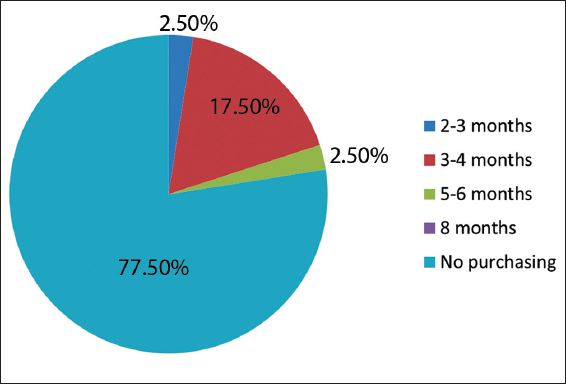
Figure 13: Duration of purchasing water
Cost of Collecting Water in a Year
Water collection cost is an extra pressure for rural people because of their poor economic condition. It has been found that 5% households spend 300–400 taka, 5% households spend 500–600 taka, 5% households spend 600–1200 taka, 2.5% households spend 1200–2000 taka, and 5% households spend 2000–3000 taka for water collecting purpose, and remaining 77.5% households do not spend money for water purpose [Figure 14]. As a result, inhabitants of 77.5% households have to suffer in various diseases due to unsafe drinking water as they are not afford to collect from a safe source.
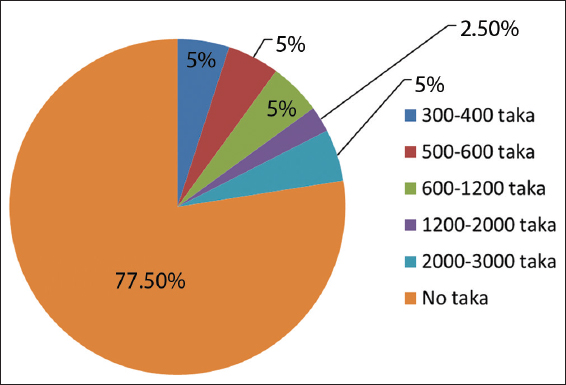
Figure 14: Percentage of water collection cost in a year
Sanitation
A standard sanitation system is a basic need in modern life as excretion is a normal physiological process. To improve public health status, the present Bangladeshi government has given top priority to rural sanitation in Bangladesh for MDG goal. However, government efforts must be ensured at all levels to achieve the improvement in the sanitation condition. Otherwise, lower standard and vulnerable type’s sanitation system can easily affect on the physical health condition of the rural people.
Sanitation System
Figure 15 shows the usual sanitation system in the study area which is grouped into improved latrine, semi-improved latrine, and low improved latrine/open defecation. From the field survey, it has been seen that about 10% households use improved latrine, 72.5% households use semi-improved latrine, and 17.5% households use low improved latrine/open defecation [Figure 16].[1-10] The present status of these latrines is unhygienic and very much lower standard. Low improved latrine/open defecation is reducing day-by-day, and this is situated near the bank of river, canal, or pond. Open defecation is responsible for spreading waterborne diseases.
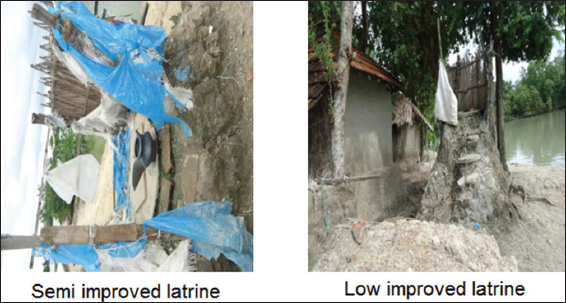
Figure 15: Sanitation system in the study area
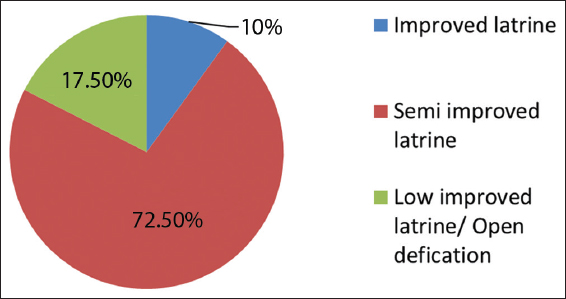
Figure 16: Percentage of using sanitation system
Main Cause of Unhygienic Sanitation
From the survey, it has been found that their sanitation condition is very poor standard because of their lower economic condition and lack of knowledge about sanitation among local people. The main cause of unhygienic sanitation is contaminated/saline water (42.5%), low improved latrine/open defecation (45%), and lack of knowledge about sanitation (12.5%) as shown in Figure 17. The aforementioned reasons are the main culprit for unhygienic sanitation.
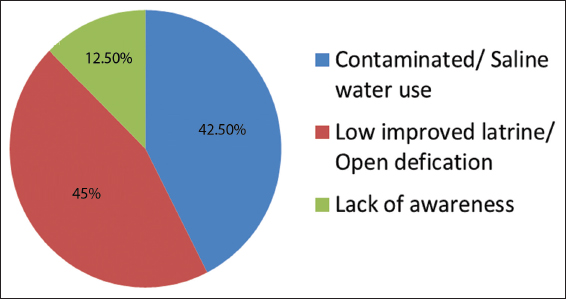
Figure 17: Percentage of the main cause of unhygienic sanitation
Health Status
Effect of saline water in physical health
Acute salinity could harm the human body and the local environment [Figure 18], and sustain here is so much complicated against rude environment, but some of them say that they are adopted with the rude environment. The effect of saline water to public health is illustrated in Figure 19.
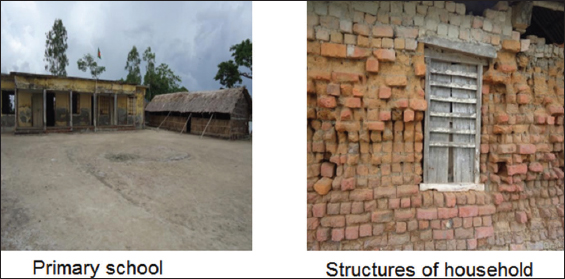
Figure 18: Effects of salinity to the local environment
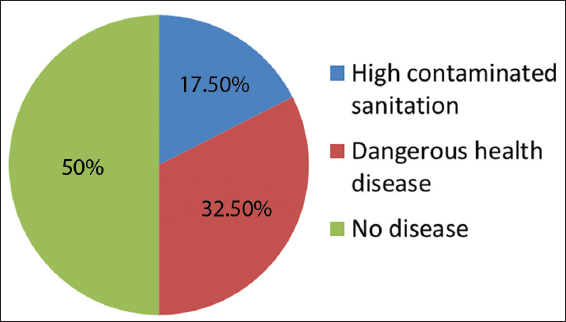
Figure 19: Effect of saline water in health
Main Cause of Diseases
90% diseases are occurred in the study area due to contaminated/saline water and unhygienic sanitation, but remaining 10% diseases are occurred due to lack of education/knowledge about health among the local people [Figure 20]. Actually, they are really unaware about saline water and unhygienic sanitation, and also they are very unconscious about their physical health condition.[6-9]
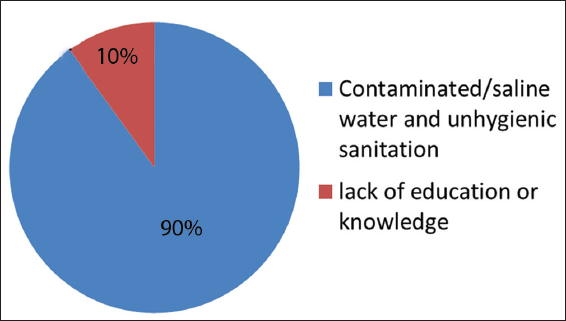
Figure 20: Percentage of diseases due to saline water and lack of education
Types of Disease
In general, diseases are closely related with water supply and sanitation systems in different aspects in the study area. Due to lower standard of water supply and sanitation systems, people are suffering severely in different diseases [Figure 21] such as 7.5% diarrhea, 5% dysentery, and 40% skin disease.[3,4,6-10] However, people are getting used to with the adverse environment with the passage of time as they do not have any alternative opportunity.
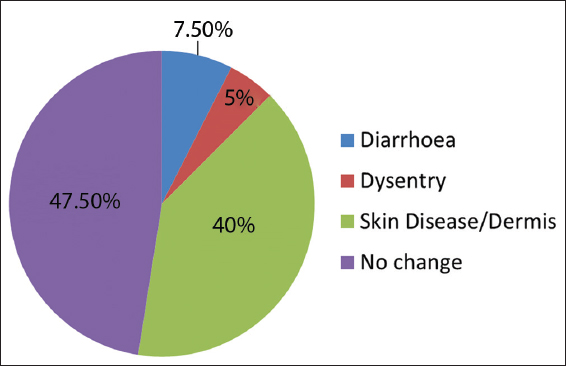
Figure 21: Percentage of different diseases
CONCLUSIONS
From the aforementioned systematic study of 40 households in the selected coastal area of Bangladesh, it can be concluded that saline water intrusion in all surface water sources is the main problem for the availability of safe drinking water. In addition, the inhabitants of the selected study area have been suffering in various waterborne diseases such as diarrhea, dysentery, dermatitis, and blister due to the ignorance about safe drinking water supply system, physical health, and environment. Moreover, sanitation system (latrine) is also very low standard in the southwestern part of Bangladesh (Nuniapara, Paikgacha, Khulna) because the people of the mentioned area have very low income and they are unaware about hygienic sanitation system. Therefore, rainwater harvesting is the only viable and affordable method to fulfil the demand of safe drinking water and hygienic sanitation system throughout the year in the aforementioned study area due to its simplicity compared with other existing techniques if some families in a group make a very big rainwater harvesting system. However, this method can be more convenient for the affected area if Bangladeshi government and different NGOs can contribute to constructing few numbers of very big rainwater harvesting system to conserve ample amount of rainwater for public use throughout the year.
To solve the existing problem in the study area, thorough awareness building about safe and hygienic living can be an effective tool to battle against the unsafe water supply and sanitation system. After all, government and different NGOs can play a vital role to encourage people for standard water supply and sanitation system for better living with necessary financial aid and education.